One of my favourite songs as a 5 year old was ‘Here We Go Round the Mulberry Bush’. I’ve been involved with the NHS for 17 years now and every winter, we do this same dance around Emergency Departments and the total mess that surrounds hospital admissions, discharges and an ever growing list of missed targets. Unfortunately, it no longer applies only to winter. It really is an absolute shambles and the problems are only too obvious. In this blog, I plan to outline them, but hopefully move away from the classic “who’s to blame” arguments and push through towards thinking about solutions…..none of which are easy, but neither are they rocket science!
So, here is a list of problems:
- We have an increasingly elderly population, who have increasingly complex health needs. You might not think this really means that much, but it has a profound impact on how long someone might need to stay in hospital and the kind of care they might require both in terms of social care and health care in the community. A recent report by the King’s Fund showed the extra strain on the health service due to a rise in people having multiple conditions is substantial. (http://www.kingsfund.org.uk/publications/pressures-in-general-practice)
- Funding cuts in social care and ‘efficiency savings’ in the NHS are having a terrible impact on hospitals and communities alike. If, as in our locality, wards have to be closed in order to balance the books, this has a massive knock on into several areas. If you close wards, it means the hospital fills up more quickly. If the hospital is full, then where do the patients who need to go into the hospital wait? The answer is in the ED. If they are waiting in the ED, then there becomes a back log of patients who cannot be seen and there will be an automatic failure to see, treat and admit or discharge patients within the 4 hour target window, which then leads to a negative rating for the hospital under CQC and pressure from on high to ‘do something about it’. But that’s just it….what can be done? Can people just be discharged home when they are unwell? – This is happening increasingly and then they end up back in hospital the next day in a worse state. The ED departments get the blame, but there is precious little they can do. At the other end of the line are people waiting to get home, but due to the deep cuts in social care, there simply isn’t the provision to put that care in place and so they are stuck. A lack of joined up computer systems between primary and secondary care makes this even more difficult. And even where patients could be cared for at home by community teams, the correct investment has not been made in this key area, hospital staff have not been trained to work in alternative environments (and believe me, they really are different) and so the teams we need in the community simply aren’t in place in many towns, cities and rural communities.
- There is a lack of information flow about patients and the care packages they already have in place and so a massive amount of time is wasted due to poor communication.
- The ‘A&E brand’ or ED, as it is now called is incredibly strong. Everybody knows it. And so people use it totally inappropriately, sometimes out of ignorance, sometimes desperation, sometimes laziness or convenience and sometimes apathy to the strain it places on services. We either have to work with this or keep on encouraging people not to use the ED. Unfortunately studies from the USA and Canada show that the more you negatively advertise the ED, the more people will use it. The King’s Fund explain with excellent clarity some of the complexities involved. What’s going on in A&E? The key questions answered (http://www.kingsfund.org.uk/projects/urgent-emergency-care/urgent-and-emergency-care-mythbusters?utm_source=twitter&utm_medium=social&utm_term=socialshare)
- Our residential and nursing home sector is in absolute disarray and in some areas of the country they are run like cartels, holding hospital trusts and county councils to ransom in terms of affordability.
- We are still unwilling to have a difficult and frank discussion about our attitude to death and how we often keep people alive for years, when we could allow them to die naturally and peacefully (I’ve blogged on this emotive subject previously).
So what happens is we have a circular blame culture in which everybody will blame somebody else, but nobody will take responsibility and so we will continue our dance around the mulberry bush! But if you have just a tiny bit of faith, you can say to this mulberry bush, “Be uprooted and be thrown into the Sea”. Where systems become oppressive and toxic, we must pluck up the complex root structure and find a new way.
Without real commitment from the government to invest rather than cut at this crucial time of transition, spending now to make huge savings in the long term, we might just continue this dance ad infinitum. The solutions cannot deliver change by the next parliament, but the transition must be honoured as vital and therefore allowed to happen over the next 10-20 years. We need a whole systems approach and it needs to involve the following (we’re trying this in Morecambe Bay):
Firstly, we need the development of Integrated Care Communities (ICCs). ICCs are geographically based, multidisciplinary teams, led and co-ordinated by a GP and a nurse but also include the vital mix of the fire service, police, mental health teams, social services, community matrons/long term conditions nurses, district nurses, community therapy teams and representatives of 3rd sector organisations. The idea of these teams to to keep care closer to home, share information, prevent admissions to hospital, but where admissions happen, ensure they happen in a coordinated way, bringing people back home as quickly as possible. We already have some great stories emerging here of this working really successfully. These teams have the potential to change the modus operandi and bring a culture change to how care is delivered.
However, these teams will fail for the same three key reasons the NHS is currently on the ropes. Resource, recruitment and IT.
These teams will be managing complex care in the community. With not too much extra funding, GPs and the care coordinators could do some incredibly effective work, but right now, general practice is at full stretch and so convincing community teams to take on this work will not be straight forward. This resource would be best invested in two areas – recruitment of staff, or retraining of staff and secondment of them from the hospital setting into the community and the strengthening of social care teams, (which to my mind are more accountable and more effective when under the same management as the NHS and provided by the state). The investment in it would also not be huge but it does involve some upfront cash. If each GP/Care Coordinator could have a laptop with Emis Web imbedded in it, with full access to their patients notes, they could go into the hospital setting once a week, do a ward round of their patients, who they know far better than the hospital teams and get them home. With the right team investment in the community this initiative would literally save millions of bed days and save an enormous amount of resource. But the better and more important benefit will be for patients themselves However, there is a warning for the government. In order for this to be effective and have the desired impact, it MUST be double-run, rather than expecting this to be done on top of what is already the status quo. The capacity is simply not in the system, but it could so easily be and this could be utterly transformational.
Secondly, the government must reverse the perverse cuts to funding. It simply bad mathematics to think that you can shrink the size of a hospital and shrink the social care provision available in the community at the same time. We need a serious reinvestment in social care. A strong and well paid social sector will bring more people into work, which btw builds a stronger economy.
Thirdly, we need to ensure all people in residential and nursing care, and those living with complex health conditions in the community have detailed care plans in place to avoid hospital admissions, except when absolutely necessary AND in line with the persons own wishes.
Fourthly, we must co-create urgent care strategies, not designed from on high, but collaboratively between ED departments, mental health teams, the police, GPs, community nursing teams and social services. If we cannot undo fifty years of public mindset about the ED, then let’s work with this rather than against it. We need more people recruited to work in the emergency setting and the pay needs to reflect the complexity and unsocial nature of the work.
Fifthly, we must stop the nonsense around data sharing, make patient records available to patients themselves and front end our EDs, Acute Medical and Surgical Units, Outpatient Departments with the same systems as we find in the GPs, all of whom should agree to share their records. In our area this would be with Emis Web, a very straight forward system to use. It would mean far faster diagnostics, more joined up, effective care for patients and investment now by the government across the UK would save them plenty of money within just a few years. It would also make data gathering, audit and governance easier and safer. The idea of spending literally millions of pounds on apps that can input data straight into patients notes, before we have this far more vital infrastructure in place is quite frankly ridiculous!
Lastly, we must work creatively with communities on public health strategies that can have a lasting impact and so stave off the growing health crises we see emerging for the future.
I don’t know about you, but to me the dance around this mulberry bush has become pretty boring, a colossal waste of time and energy and so in my opinion, we should quite simply stop it and do something different. The solutions are right in front of us. Will the government have the guts to stop what they are doing and make the right investments now for the sake of the health and wellbeing of the population at large and the health and social care system as a whole. They might not get the glory at the next election, but in ten years time, we will see that the right choices were made for the good of all.

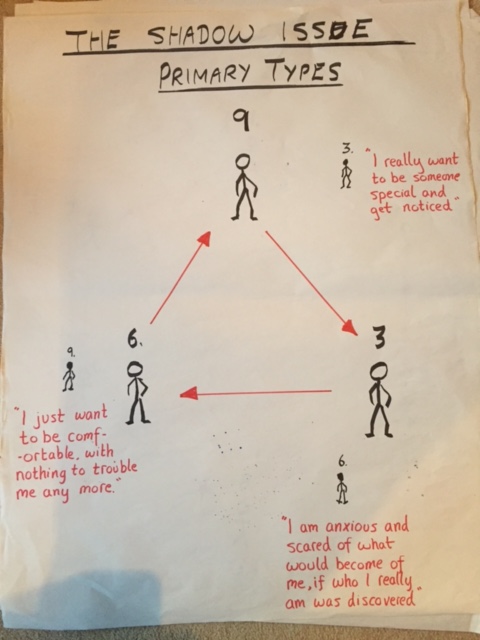 So, focusing in on the UK (maybe some thoughts on the lovely USA another time), if we are to shift the political discourse towards something more healthy for the future, we need to learn to listen to the part of us that feels the need to be safe. We need to understand the ‘shadow’ part of our corporate personality that is anxious and fearful, admitting to ourselves what drives our thoughts and actions. When a Type 6 personality is not in a healthy place, they will begin to regress into a Type 3 pattern of thinking. So, the underlying drive to be safe becomes the need to get noticed and be special. So, post-brexit, some of which was about the need to be safe, we find our politicans trying to re-assert our Soverignty and our ‘Greatness’. Only a couple of weeks ago, Boris Johnson, the Foreign Secretary, was declaring on the radio that we don’t realise quite how the rest of the world sees us. Apparently, they admire us and think we need to continue showing great leadership in the world. We continue to believe this about ourselves, that we are very special and have a vital role which the rest of the world needs us to play. I wonder if we actually asked the rest of the world whether or not this is true, they might laugh in our face, pat us on the head and gently remind us that the world has moved on, but maybe we have not.
So, focusing in on the UK (maybe some thoughts on the lovely USA another time), if we are to shift the political discourse towards something more healthy for the future, we need to learn to listen to the part of us that feels the need to be safe. We need to understand the ‘shadow’ part of our corporate personality that is anxious and fearful, admitting to ourselves what drives our thoughts and actions. When a Type 6 personality is not in a healthy place, they will begin to regress into a Type 3 pattern of thinking. So, the underlying drive to be safe becomes the need to get noticed and be special. So, post-brexit, some of which was about the need to be safe, we find our politicans trying to re-assert our Soverignty and our ‘Greatness’. Only a couple of weeks ago, Boris Johnson, the Foreign Secretary, was declaring on the radio that we don’t realise quite how the rest of the world sees us. Apparently, they admire us and think we need to continue showing great leadership in the world. We continue to believe this about ourselves, that we are very special and have a vital role which the rest of the world needs us to play. I wonder if we actually asked the rest of the world whether or not this is true, they might laugh in our face, pat us on the head and gently remind us that the world has moved on, but maybe we have not.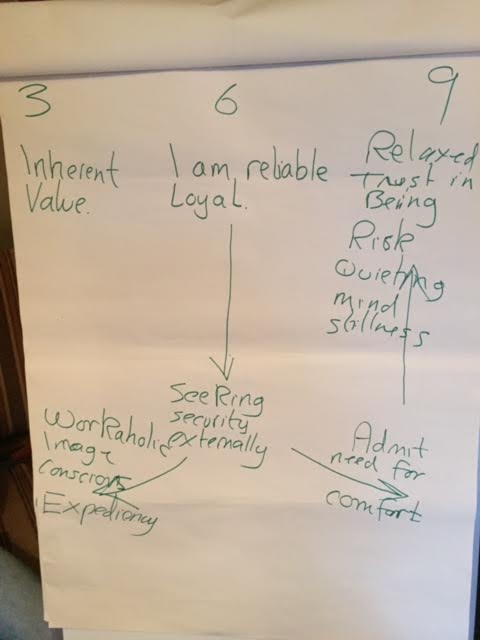
{kind=link}
{kind=link}
){kind=link}
{kind=link}
{kind=link}