“Of all the skills of leadership, listening is the most valuable — and one of the least understood. Most captains of industry listen only sometimes, and they remain ordinary leaders. But a few, the great ones, never stop listening. That’s how they get word before anyone else of unseen problems and opportunities.”
— Peter Nulty, Fortune Magazine
Here in Morecambe Bay, I’ve had the privilege of hearing Trina, a brilliant member of the community in Morecambe, give her testimony to Heidi Allen MP and Frank Field MP from the select committee for the Department of Work and Pensions, and more recently to the Chief Medical Officer, Prof Chris Whitty, when he visited the Bay. Trina is an amazing woman. She keeps a freezer full off food in her front room to feed members of her local community who are on the ropes or have been sanctioned. She knows what it is to live with the experience of poverty and the complex issues involved. I love the way in which she fearlessly speaks truth to power:
“Ending up on benefits isn’t always as simple as losing your job. It can be the result of bereavement, illness, injury, or a breakdown in a relationship. It’s a culture shock. For me, one day I had a grand a week coming in. The next day I was applying for IS. It took 14 weeks for my payments to come in. 14 weeks where I still had to pay the rent, pay bills, feed my child. You default on anything on a contract. Worry about it later. And you sell all your ‘nice things’ for pence, to keep a roof over your head. Then the fridge breaks – or the cooker, or the washer – but you’re still only getting your IS payment, not housing benefit or tax credits. It’s different now, it’s all UC – but that’s harder, coz it’s all rolled into one so you don’t even get that small amount of IS. With no other option (you can’t get normal credit) you go to Brighthouse (or the current equivalent) or you get a loan from Deebank/Provident/Greenwoods. You pay 4x as much back in total, but it’s only £5 per week. Your credit rating gets worse because you’ve defaulted on all your ‘luxuries’ – contract phone, sky tv, landline phone. Debts become bailiffs knocking on your door, and if you hide from them long enough… county court judgements. You’re still trying to learn to re-budget on less than 30% of what you used to have. All whilst dealing with illness, bereavement, disability, or social workers on your case because you were a DV victim and the police involved them. You move house because you can’t afford the rent. Then you’re sanctioned. Because despite telling the job centre three times that you’ve moved, they sent your appointment letter to the wrong house. Or you were in hospital. Or your child was sick. You appeal, but they uphold the sanction. You try to re-budget again. Your ex-partner decides they don’t want to bother with the kids anymore. So they stop paying child support and disappear. The CSA/CMS ‘can’t find them’ despite you providing their address and phone number. You try to re-budget it again. If that doesn’t make you think twice about judging people in poverty, consider going through that – which was my experience in 2009 – in the midst of a global pandemic, when there’s no jobs, food has gone up 60% you’re frightened to leave the house in case you get sick….And the world and his wife are taking to social media to espouse how you’re a shit parent and need your kids taken off you, because no matter how hard you try to explain that you’re not a scrounger, they tell you that you should use your non-existent money to just make soup.”
Trina’s experience is replicated thousands of times over. And whilst national leaders tell us they have already done enough and it’s not their responsibility to ensure that children are fed, let us examine these claims, with some help from the BBC.
The BBC ask – How much money is the government spending?
By BBC Reality Check
“Earlier, when pressed on free school meals, the prime minister told the BBC “there’s £63m specifically to help deal with holiday hunger and with pressure on families,” referring to payment made to local authorities in June.
However, the £63m was for a “local welfare assistance fund” to “assist those struggling to afford food and other essentials” and was not just to feed children.
Guidance for the funding stated that the government “anticipates that most of the funding will be spent within 12 weeks”, meaning that it was expected to have been spent before the end of September.
In England, about 1.3 million children claimed for free school meals in 2019 – about 15% of state-educated pupils.
Analysis by the Food Foundation estimates a further 900,000 children in England may have sought free school meals since the start of the pandemic.”
SO – just to be REALLY clear – the £63 million the government are talking about has ALREADY been given to councils (in August) and has ALREADY run out (as by the government’s own admission it was only expected to last for 12 weeks from the time it was given). It amounted to 34 pence per child, per day (the maths is fairly straight forward – £63million, divided by £2.2million – the number of children now needing Free School meals, see above facts from the BBC and then dividing this amount by 84 days – that is the 12 weeks for which the funding lasted). The government keep saying that they have funded councils to fund FSM vouchers, but a) this is no longer the case – the money has run out (as the Conservative Leader of Warwickshire County Council informed the government) AND b) it was woefully insufficient anyway to provide adequate nutrition! This all matters because the government are telling us that they are doing enough, but they plainly are not.
The things is that most of us find it hard to comprehend the difference between a million and a billion pounds, because we never encounter that kind of money. I find this graphic from reddit really helpful because it demonstrates it in a simple form. £63 million sounds like a lot of money, until you compare it to the £12 billion the government have spent on an ineffective test and trace system. They seem to be able to find massive funds for public health schemes which are failing, on the one hand, whilst unable to do provide sufficient funds for programmes that we know make a very real difference, you know – feeding hungry children.
With food bills possibly set to rise as the prospect of a no-deal Brexit becomes all the more real, the problem of hunger, not only for those already in poverty, but for many more families, currently just about holding it together will be felt ever more acutely. History teaches us that widespread hunger leads to civil unrest and sometimes even revolution. Now is not the time to remain entrenched in ideology. Now is the time for humble listening, and a change of heart. When the people are unable to buy bread, beware of the detached and senseless arrogance that cries, “Let them eat cake!”
I love Marcus Rashford! His statement on child hunger is brilliant, but I don’t entirely agree with him. In his impassioned plea for us to take child hunger seriously (which I could not agree with more), especially through the school holidays, he says: “this is not politics, this is humanity.” The reality is that EVERYTHING IS POLITICAL. Politics is about how we see the world and how we live together. Economics is about how we share and manage the resources between us. Child hunger and child poverty IS a political and economic issue! We can’t hide away from this. We can call for political unity over the issue, we can appeal to the deep compassion of the human heart – but we cannot try and de-politicise the issue, however hard we try. Nor can we remain silent, in case it looks like we’re playing party politics. I am not associated with any political party. None the less this is a deeply political issue – political with both a small p and a very big one!
Listening to the debate in the House of Commons about whether or not children should be given meals, provided by the state, during the school break, there seemed to be four main objections to the idea proffered by some of the Conservative MPs.
Rather than give children meals, thereby nationalising them, we should be actively promoting parents to take more responsibility, rather than being absent and encourage them to provide for their children properly. We need to deal with the causes of the causes.
The state is already giving out quite enough help already, thank you very much, via Universal Credit.
We’ve all got to play our part in helping out. We’ve had ‘eat out to help out’ for the rich, now we need ‘eat nowt to help out’ for the poor…..(slight tongue in cheek point, perhaps….)
Let’s just examine these from both a population health and social justice perspective:
Well….I don’t know of very many parents who don’t want to ‘take responsibility’ for their children’s wellbeing. In fact there is hugely weaponised stigma and societal shame (wrongly) applied to those who can’t. There is a massive difference between not wanting to and not being able to. I don’t disagree that we need to get to the causes of the causes of poverty and child hunger – absolutely right! But this will take a generational, focused, gargantuan and sustained effort and will involve us turning the tide on: Adverse Childhood Experiences, an unbalanced and unequal education system, spiritual and psychological degradation, ingrained and systemic racism, white privilege and abusive patriarchy, county lines, unaffordable land and housing (both to buy or rent), poorly paid work, a broken justice system (over 300000 children have at least one parent in prison) etc. We should definitely work on all of this! And as we do it will enable people to be able to take more responsibility and make more positive choices – I’m all for that. Unfortunately at present, the reality is that there are far fewer real choices available for people living in our most economically deprived communities. This is not about either/or – it’s about both/and. So, in the mean time, whilst we’re working on the causes of the causes, perhaps we could also guarantee that we don’t perpetuate the cycle further and ensure children are fed?
The idea that by the state stepping in it encourages dependency, fecklessness and laziness is actually ridiculous. State intervention to provide for the hungry would actually show that we have a society and a government who care deeply for people who are struggling and having a hard time. It is one of the great debates about the role of the state, but the sad reality is that charity alone, simply won’t cut it. We need a state (be that city, regional or national – preferably all), that acts as a safety net for those who are finding life the hardest. Rashford puts it best: “……since March, 32% of families have suffered a drop in income. Nearly 1 million have fallen off the payroll. This is not dependency, this a cry for help. There are no jobs!! 250% increase in food poverty and rising. Nobody said this was simple…” Until we fix the causes of the causes, we are going to need to ensure we have appropriate interventions to the difficult realities so many in our communities face. Perhaps this might include children being fed through the holidays?
Despite the ‘positive changes’ to the benefits system, with more people in work, we had rising poverty levels even before the pandemic, with more children in poverty, (worsening over the last ten years) and now we have massive job insecurity, higher Rise in use of Food Banks – Trussell Trust
unemployment and we’re heading into a recession. At such a time, to imply those benefits are enough, when we know that the use of foodbanks (which are supposed to be a temporary measure) is rising, is somewhat short-sighted. I have heard so many testimonies of families who are on the ropes. Holiday food vouchers are a life line. However good you might think your benefit system is, when families are telling you they are having to choose between fuel and food as we head into winter, perhaps we might want to think about how we ensure children are fed? After all, nutrition is one of the key building blocks of a healthy and well child.
It is simply inhumane to ask the poor to fit the bill of the ill thought through spending of public money over the previous several months. There have been some VAST pay outs (which will indebt the very children the government are refusing to feed) to many companies, with clauses protecting them should they not deliver on their contracts, (which is lucky for them, because they have failed, badly)….and yet we can’t find the money to ensure that children are fed. One might wonder whose side the government is on.
I make no secret of the fact that I am personally deeply motivated by the politics of Jesus. There are two really clear things that he had to say on the issue.
“I have come to preach good news to the poor” (Luke 4v18-19) – and he backs this up by stating that He will restore ‘Jubilee’ – this is a radical economic redistribution of money and resources, to the poor, to combat greed and bring things back onto a level playing field.
“Let the children come to me, for to such belongs the Kingdom of Heaven” (Luke 18v16) – Not only are we to care for children, because they are important – we’re supposed to become more like them (Matthew 18v3)!
In other words, if the politics of Jesus are to be taken seriously (and it seems that many conservative voters and MPs profess a ‘Christian’ faith), let it be noted that according to the Christian faith, the poor, the hungry and children really matter to God! And yes – there is space for the church, other faith organisations, charities, communities and local leaders to step into the gap and ensure children are fed, despite the government’s response – but there is also a ‘prophetic mandate’ to challenge injustice and hold leaders to account. The truth is that the need is great – 1 million children across the UK will be hungry over October half-term – they don’t want this to be ‘relooked at for Christmas‘ – they want their bellies fed now. The national government’s arguments fall flat. While children go hungry, they find themselves defending their senseless ideologies and punishing the defenceless. They urgently need to change their minds!
The winter hasn’t even hit us yet. But it will and it’s going to hit us hard. Harder than we know. Harder than we are prepared for. Do you remember January 2015, with queues of people lying in corridors in our Emergency Departments, and a high spike in winter deaths? One of the people I respect most in the world of Public Health, Prof Dominic Harrison, highlighted to me this week, that it was a three-fold, intertwining cord which led to the devastating outcomes: an ineffectual flu vaccine, high staff vacancies in the NHS, and high staff sickness rates. But here’s the thing – this year we have more factors (Covid-19, incoming Influenza, staff gaps in the NHS, people having to self-isolate and sickness levels rising – this week our surgery had 14 staff off with C-19) and although, so far we haven’t seen the spike in deaths associated with the rising number of Covid-19 cases (thanks to better treatments), our hospitals are filling up fast, whilst the mantra remains, that the NHS must get back to pre-Covid levels of operation. This is going to be a tough winter. And it’s going to be worse, as it always is in our most deprived communities, which will further widen the health inequalities gap. And people are going to die, not only of Covid and influenza, but of other preventable things like heart attacks, strokes and suicide, in higher numbers than usual. What am I, a prophet of doom? Well…..I hope not! But this is a wake-up call.
It’s no surprise that so many people feel a smouldering sense of anger towards the government. There is no doubt that things could and should have been handled differently from the beginning. It’s no use saying – well….we didn’t know what we were facing, we weren’t prepared for this….. the government didn’t even follow their own advice from their preparedness exercise three years ago, they have outsourced test and trace to companies with no track record or expertise in the world of public health to the tune of £12billion and it doesn’t even work effectively. They have given contradictory advice to different regions of the UK, they have continued to allow foreign travel, they have failed to adequately explain the reasons for certain policies which key members of their inner circle haven’t even followed, they have briefed key city leadership teams through the press and failed to win the public’s trust – something which is so crucial at such a time as this. They have “followed the science” and then not followed the science…..it has been a shambles and it’s no wonder that people are disengaged.
HOWEVER – this is not the time to let our cynicism get the better of us! What we have to face is that we are where we are and we’re heading into winter, and our anger towards these various failings is in danger of causing us to embrace apathy or rebellion – both of which will have terrible consequences. So right now, we need to keep our heads and we need to take a deep breath. There will come a time for the government to answer serious questions about how they have handled this pandemic and the decisions they have made. But it is not now. Now, we need to look ahead and be really pragmatic about what we’re about to face together.
Ensure the Test, Trace and Isolate system is robust. Test results need to be back within 24 hours, 80% of contacts must be traced and strict adherence to the 14 days isolation is vital. The current system still isn’t working effectively enough, despite an eye watering bill with no sense of accountability or responsibility for it’s failure. It is not too late to ensure that local directors of Public Health can lead this work heading into winter and ensure that all available labs are put to effective use.
Solid, consistent and clear public health messaging needs to go to the public through every means possible. There needs to be rationale and helpful explanations about why certain measures are being chosen.
We need strict border measures to stop the virus from re-circling.
Secondly, as the public we need to take whatever responsibility we can to ensure we continue to do all we can. Conspiracy theories are not even vaguely helpful right now. And although it’s true that death rates have been lower than expected, there are other things to consider. This is still a dangerous virus – it will lead to many extra admissions to hospital through the winter period, especially linked with Respiratory Illness and it will affect unsuspecting and previously healthy people with the effects of long-covid – I have seen the effects of this in my (young and previously fit) patients and friends and it is truly debilitating. With all the other things we have to cope with this winter, we can’t afford to let our guard down – not now. We know from public health data that the vast majority of spread is between family, friends and neighbours. We also know that it won’t just be Covid-19 that kills people this winter. Higher than normal deaths from other illnesses/conditions are expected across the board. So, here are some sensible things we can all do to try and stay well:
Have a flu jab if you’re in one of the ‘at risk’ groups
Take worrying symptoms seriously! Don’t ignore chest pain (especially if it’s worse when you exert yourself), or new lumps and bumps – especially in your more private parts, or bleeding from somewhere you don’t normally bleed from, or unexplained weight loss. See your GP!
Wash your hands regularly
Wear a face mask when out and about
Spray and wipe down surfaces
When you cough or sneeze, do so into your elbow crease
Keep 2 metres apart from people who are not in your household, and wear a facemask if you have to get closer
Keep within your household bubble – the vast majority of spread is now happening between family, friends and neighbours – we can’t be blazé about this!
As far as possible (recognising that choices are significantly reduced for many of our communities), make good choices for your own physical and mental health:
Eat well – be determined to fuel your body with good nutrients – if you’re trying to get to a more healthy weight then significantly reduce salt, alcohol, sugar and carbohydrate in your diet. Consider taking a vitamin D supplement through the winter – 1000units daily – only about £1 for 60 tablets from most pharmacies.
Exercise – this doesn’t have to be anything unrealistic or intense – stop looking at other people’s sculptured bodies and feeling crap about yourself. You are beautiful! Just take a walk, if you’re able, every day – whatever the weather, and get some fresh air. If you’re unable to walk, try some gentle chair-based exercises – it doesn’t have to be anything heroic – something is better than nothing. Do more if you want, but let it become enjoyable, rather than a chore – something you’re choosing in order to make life better and more happy.
Be grateful – everyday, when you wake up and before you sleep – try and think of three things you can be grateful for that day.
Breathe deeply and use breathing techniques to calm yourself down, like box breathing (breathe in for 4, hold in for 4, breathe out for 4, hold out for 4).
Connect with people – even if it’s via zoom, facetime or the phone – whatever it takes – connect with other human beings around you. Social isolation is literally a killer. We must take care of each other. Ask people how they are and genuinely care enough to listen. Some people are going to tell you they aren’t sure they want to carry on living. Ask them if they are thinking about ending their life. If they say yes – ask them if they have made any plans. Either way, take this seriously. Help them get help. Ask them if they have phoned their GP yet. Tell them you’re going to to keep walking with them through this tunnel. Reassure them that there is a light even though they can’t see it right now.
Learn something new – a language, a skill, whatever you fancy – give it a go.
Relax – seriously switch off the 24 hours news cycle, disconnect from too much social media and take time to do things which are good for your soul – sing, dance, read, play games, take long baths, whatever helps…..
Sleep – our bodies and our minds regenerate when we sleep. Sleep is good!
Above all – keep love and hope alive. We’ve got to dig deep to keep loving each other – being kind in our attitudes, even towards our enemies. And keep on keeping on hoping. If you’re not sure how, this podcast with Brené Brown and Michael Curry will help!
Thirdly, the NHS is not yet ready. Yes – there have been some remarkable things which the NHS has done to respond to the first wave of Covid. Contrary to some misleading articles about General Practice, we are and have always remained open and available to our patients. We are triaging all patients via the phone to work out how we can best help and employing loads more technology to help us do this. It’s so much better for a young mum of three kids to be able to have quick video-call about one of her children’s rashes than have to lug them all down to the surgery. It’s great that we can now supplement a phone/video call with an advice sheet sent to your phone. It also means that we can prioritise who really needs seeing face to face and keep our premises as Covid-secure as possible. Many community staff were redeployed from their usual work, such as Speech and Language Therapists, Occupational Therapists and Physiotherapists, into the Nightingale and Rehabilitation hospitals, meaning they were taken away from their usual work, with a huge amount to now catch up on. This was not without cost to families who needed their support or were awaiting a diagnosis, and added to the strain in General Practice also. It was tough. But it was worth it. And we’re so grateful for the way the public were overwhelmingly understanding towards us as we tried to flex our services to cope with the demand.
However, we need to take a radical stocktake of where we are and again put into motion some very different ways of operating over the next 2-4 weeks. It will allow us to work in a way that is safest for the public and will provide a sense of reassurance. Although I welcome the reopening of the Northern Nightingale Hospitals – as usual, the focus is far too much on the Acute Hospital sector and not enough on how we can help people stay more well in the community and prevent admission, particularly in our economically poorest communities. It’s important that the public understand that we need to reorganise our services in the community again in order to try and enable as many people as possible to stay well through this winter, particularly in our poorest communities, where admission to hospital and early death rates are always significantly higher.
I have nothing but compassion and camaraderie with GP colleagues as they cope with a huge surge in demand, (just indeed as I do with all NHS workers and carers right now, whatever their role). What I believe we need to do NOW though is change the way we’re working so that we can give real focus into the areas which are likely to affect people’s health most significantly over the months ahead, support our community colleagues to focus on various aspects of their work more effectively and enable our teams to be resilient and stay well themselves through the winter, whilst serving the communities with their usual brilliance. Here are my suggestions, which we are exploring in more depth across Morecambe Bay and indeed our Integrated Care System across Lancashire and South Cumbria (though important to note that this is more about function than form, so might ‘look’ different in each locality):
accept now that we cannot get back up to pre-covid levels of activity, for example in routinely scheduled operations, and if we try to, it will lead to more unnecessary deaths. This is a big ask for people who are waiting for their hip to be replaced, or their hernia to be repaired, but we have to be realistic about what is possible with the resources we have available.
re-focus and align existing capacity in order to ensure a more coordinated approach to addressing demand.
target additional resource to mobilise capacity where it will have the most impact.
use data and evidence of risk and vulnerability from COVID-19 in a more systematic way to inform a response that is scaled appropriately.
In order for this to work practically, we must create a model which makes this possible. Perhaps one way is by reorganising into a model of Red, Amber and Green Community Hubs, supported by a co-ordination centre, which pulls together the data and brings aid when practices are struggling, could work in the following way and allow us to work as effectively as possible (recognising that this may vary according to Primary Care Network/ICP/MCP need and capability/capacity):
Red Hubs (which can be remote in terms of triage) staffed by Paramedics, GPs and Nurse Practitioners, to deal with COVID-19, Flu, and Acute Respiratory Illness (i.e. anyone with a fever, cough or breathlessness). It may be that out of hours providers may already be in place to supplement and support this model.
Amber Hubs – a remodelled care co-ordination team approach led by the General Practice Team with proactive support from community (including mental health) teams. They would use an asset based community development model of Population Health Management and work WITH communities to:
Focus and drive on proactive long-term condition management AND other acute illnesses that don’t fit the criteria for the red hubs.
Have a driving focus on proactive long-term condition management with particular emphasis on conditions more vulnerable to poor outcomes from COVID-19.
Be supported by redeployed medical specialities.
Fund and support the Community Voluntary Faith Sector to partner with Primary Care and Community Teams to create a really resilient partnership in doing this work together, recognising the HUGE impact the 3rd sector makes to this work and how fragile they are in terms of adequate resources.
Be sited so as to ensure accessibility to residents within the 20% most deprived communities within each ICP/MCP.
Have attached to them place based multidisciplinary assertive and active case management and care co-ordination teams (think spokes) as outlined previously. These teams would have a focus on the “priority wards” and groups experiencing higher levels of social isolation.
Take a “more than medicine” approach by having active in reach from other partners reflecting broader, social needs that are barriers to improved health and wellbeing; social prescribing, housing, employment and more as informed by the data.
Cardiovascular Interventions
Hypertension – we have too many patients with a BP >150/90 (current guidance shows we should be aiming for <135/85 for the general population and <130/80 for those Diabetes or known heart disease). We will best prevent MIs and CVAs by being much more proactive in this area.
Atrial Fibrillation – ongoing protection work by ensuring appropriate anticoagulation in those with a Cha2ds2vasc score of over 2.
Diabetes (and Cancer)
focus on healthy weight, driving down BMI where possible, through targeted interventions and
reducing HbA1c in people through targeted lifestyle interventions and medication where necessary.
Respiratory Disease (and Cancer)
Stop Smoking interventions
Weight loss programmes
Winter warmth schemes in homes and damp removal – this will be vital in keeping admissions down
Cancer – Getting a real focus on 2 week wait referrals with appropriate messaging to the public
Mental Health – Suicide Preventions
Mental Health reviews
Targeted messaging to the public to help them understand why and how things are changing
Suicide awareness training
Frailty and Care Home work – ongoing support and focus on the frail and those in care homes
Green Hubs – these will focus on:
Musculoskeletal problems – physio first and possible redeployment of Orthopaedic Surgeons and Pain Specialists, to run clinics and provide joint injections in the community rather than surgical procedures, to see people through the winter period
Other day to day, essential General Practice issues – baby checks, smear tests, dermatology, rheumatology, ENT, low level mental health etc – run by a reworked and repositioned team
The model above won’t work for all, but the principles are important. It might all seem a bit radical and it’s true that there would need to be a significant amount of resource and support flowing into the community to enable this – however, if we don’t do something like this, then it’s like knowing an earthquake is coming and not bothering to take aversive action. We don’t have the personnel we need right now, but partnering with the voluntary sector (with appropriate resource allocated) and ensuring we have the right data help and support will make this more possible. Finances must be freed up to support this model and NHSE need to give the ICS teams across the nation some slack to take this more proactive approach. It will actually lead to huge savings (of lives and money).
We’ve already lost a lot of people to Covid-19. We’re heading into a serious economic catastrophe and a winter of discontent. Good public health and good health care IS good economics. If the government heed the warnings, if the public take this seriously and work with us, if the NHS can reorganise, even at this late stage, then we will significantly improve our chances of getting through this winter well together. We won’t have another opportunity to ‘get this right’. I hope we will act now and find that we really can make it through together.
“Talk is cheap” – my Dad used to say this to me, if I told him I was going to do my chores but didn’t do them. It was a fair challenge to my teenage self! It’s ok to have good intentions, but if we don’t act to back up what we say, then our words are meaningless. One of my most recent blogs explored what we can do to tackle poverty and health inequalities. One of the things I didn’t focus on, but which deserves a blog all to itself is the inequality caused by and the social injustice which is perpetuated by the funding formula used within the NHS. I will demonstrate, using a few examples why this formula is so antiquated and suggest that the ‘Morecambe Bay Formula’ which we have developed might be a better model for the future if we want to put our money where our mouth is! I’m sure with Boris Johnson’s ‘levelling up’ agenda, that the time has come for us to take this seriously.
The current Carr-Hill Formula takes into consideration various factors. Generally it’s what we call a weighted-population formula and distributes money and resources according to various complex factors but puts insufficient weighting on the issue of deprivation. What this means in practice is that wealthier areas (like the South East) have significantly more money, per head of population, spent on them than areas (like the East Midlands or the North West), where poverty rates are much higher and health outcomes are significantly worse.
Let me give you two examples from here in Morecambe Bay as to how that makes little or no sense if we are serious about levelling up.
Here are a couple of graphics showing how life expectancy changes along two different bus routes around Morecambe Bay (recognising that these are averages within these towns and are significantly worse within some more localised wards):
You can see the stark differences in life expectancy between people who live in Barrow-in-Furness and those who live in Ambleside, or those who are in Heysham compared to those in Levens. People in our areas of 10-20% lowest Index of Multiple Deprivation (IMD) are dying 10-15 years earlier than their counterparts in our wealthiest wards. Surely we care enough about this to want to change things?!
So, our team did a little exercise in which we thought together about how we might spend £500k, if we were going to try and ‘level up’. Our Bay, is broadly divided into three districts. The Furness Peninsula, South Lakeland and Lancaster District (which is basically North Lancashire). We divided the area up according to the lowest 10% IMD and distributed the money accordingly, knowing the kind of projects we could invest in to make a difference to people’s life expectancy and wellbeing. The results were stark! We found that out of £500k, we would spend around £232,000 in the Furness area (predominantly wards in Barrow and Millom), £267,000.50 in Lancaster District (predominantly Morecambe/Heysham and some wards of Lancaster) and just under £500 in South Lakeland! £500 out of half a million! But that’s how stark the differences are in our Geography of around 1000 square kilometres. When we then changed this formula to be based on our lowest 20% IMD areas, the South Lakes still only ended up with just over £1000.
We’ve also recently done a review of how many people in each area are living with Long Term conditions. What is very interesting is that in two almost identical areas in population size (Lancaster and Morecambe), but one with significantly more areas of increased deprivation (Morecambe), people in that area have a higher number of Long Term Conditions (LTCs). However, when it comes to the allocation of resources into the Primary Care Networks, working in these two areas, this is done on the size of the population, not the complexity of what those populations are dealing with. So, even though there are far more people living with multiple LTCs in Morecambe, compared to Lancaster, they are both allocated the same number of staff through the PCNs to deal with their relative problems.
This means that areas like Morecambe and Barrow are missing out twice over. They are not getting the money into their areas in the first place to allow them to level up on the ’causes of the causes’, as Sir Michael Marmot puts it, – i.e. they are not able to get into good preventative public health AND they are not given a fair weighting when it comes to helping those who are already living there with significantly more complex health needs. This means teams working in places like Morecambe can find it harder to recruit and their teams can suffer easier burn out, or are simply unable to provide the help to their communities that is needed. We know that economically poorer areas have higher populations of BAME citizens also, which is vital to understand if we’re serious about ‘Black Lives Matter’.
This injustice needs to stop if we are serious about tackling health inequalities. Talk is cheap. It’s time to put our money where our mouth is. We can’t just talk about levelling up, we must do it! We need action and that action needs to take the form of a recalculated funding formula, which ensures that the communities that need the most help are able to get it. When it comes down to it, I’m a pragmatist. There are pockets of poverty, even in our wealthiest areas and issues like frailty can make the provision of care more expensive (though one could argue that in poorer areas, we’re dealing with frailty 10-20 years before it is seen in wealthier populations). So…..we need to do two things:
We need to change the way funding is given through the Primary Care Networks to ensure that those who have the greatest task, get the greatest help. This needs prioritising by the national leadership team.
We need to ensure that we create a funding formula from the National Team into the Integrated Care Systems in each of the regions and then within each ICS that recognises the complexities we’re dealing with when trying to level up. The funding formula based on IMD (either lowest 10 or 20%) is indeed quite extreme – perhaps it needs to be. Perhaps a more realistic formula is to to weight it 50:50, with half of it calculated according to the lowest 20% IMD and half according to the Carr-Hill Weighted formula. This has gained broad support across the board in our part of the world. We call it the Morecambe Bay formula (though it is with huge thanks to Mark Wight and Anji Stokes!). We believe it is far more socially just.
Over the last 18 years, I’ve been journeying with the help of the Enneagram – although I would say I’ve taken it more seriously over the last 6-8 years. I have found it to be utterly transformational in how I understand myself and how I can become my best self. I would recommend it to anyone and everyone – it is honestly the best tool I have ever found for personal/spiritual development, and how to live well in human relationships. The hard reality is this – if we don’t do our (inner) work, we will never change. I think it’s also true that understanding our own personality type and those of other people allows us to be much more focused in therapeutic and medical interventions. I hope this blog helps us to get to some of the root issues in our personality types that can cause us to sabotage ourselves then it comes to living well in our bodies.
Your Personality Type
I have personally found the Enneagram an incredibly helpful framework for understanding how the the human personality develops and why we behave and think in the ways that we do. The teaching is ancient and sacred and I am certainly no expert. There is absolutely no way that I can even begin to do justice to this wisdom in such a short blog, (although it is something I will continue to explore in future posts and podcasts), but I hope some of my personal reflections on what I am learning may be helpful by way of introduction. In short, the wisdom of the Enneagram teaches that there are 9 basic personality types or ‘ego-projections’. In response to encountering the environment around us as we grow, our personality develops around our deepest unmet needs and root struggles/’sins’. This is our ‘false-self’. If we are not awake to who we are and how we function in the world then we will not understand why we continue to behave in certain ways and trip up over the same issues again and again. The gift of the Enneagram is that it doesn’t define who we are are and what we will be. It helps explain why we’re stuck in the box we are in and helps us break out of it, so that we can be become more fully who we really are. Over time, as we develop and do our work, we are less obviously one number or another and begin to become more whole. The Enneagram invites us to surrender ourselves (to God, as Richard Rohr clarifies) and let go of the need to keep up the pretence of the ‘false-self’ we have created to protect us and/or impress others and instead to become our true selves and a true gift to others.
There are two main traditions within the Enneagram teaching. they have some similarities and some differences in their understanding and application of The Enneagram:
Enneagram Worldwide (which is what I know more of) and The Enneagram Institute. Their websites are great resources:
If this is something you decide to explore I would REALLY recommend that you don’t take an online test. Read or listen to some stuff first – take notice of your responses to the various types. There will probably be two or three types that you might associate with, after you’ve got your head around some of the basics. Read/listen around those types first and THEN take a test or two, if you’re still not sure. I really like what Richard Rohr says when he mentions that the type that you most react to may well be the type that you are! Often it is uncomfortable for someone to hold a mirror up to us.
Let me just offer some brief insights on each type to whet your taste buds and see if this might be something that helps you, or alternatively, stop reading here and either buy the books or disengage with this idea completely! I am particularly grateful to my incredible Enneagram coach/therapist/friend/spiritual mentor, Paul Wood for helping me in my own understanding and growth.
Before we delve into the nine ‘types’, it’s worth saying a quick word about the three triads and the three sub-types!
Each of the Enneagram types is divided into groups of three. The head types: – fives, sixes and sevens; the heart types: – twos, threes and fours; and the body types: – eights, nines and ones. As a doctor, I am fascinated by disease and although I haven’t seen any research into this yet, I think it would a fascinating area of research to understand how the various types affect physical health conditions. There are definite links with certain mental health conditions and some personality types are more prone to develop certain ‘personality disorders’. Perhaps more on this another time!
The Enneagram also teaches that for each of the 9 personality types, there are wings and also 3 sub-types – social, sexual and self-preserving. For those of you who know the Enneagram, I’m not even going near the wings in this blog! The sub-types though, are pretty important because they can make people of the same type behave pretty differently.
Each of us has one dominant sub-type, one secondary sub-type and one ‘blind-spot’. One of these best ways to think about it is this: if you walk into a room full of people, with a buffet on one side of the room, what do you do (other than walk straight back out again – type 5!?!)? If you work the room and like to make lots of contact with people, you’re likely a social sub-type. If you make a beeline for the buffet whilst checking out where the exits are and ensuring you stand in a place where you will feel most safe, then you are likely a self-preserving sub-type. If you are trying to work out who the most interesting person in the room is, with whom you could have a really in depth and personal conversation, then you’re likely a sexual sub-type. I, for example, am a social sub-type, with a secondary sub-type of ‘sexual’ (or I prefer the term one-to-one), but my blind spot is ‘self-preservation’. What that means is that I love to have lots of company, go to lots of gatherings, usually where there is lots of food, with which I tend to overindulge (out of politeness, of course), and I have a great time working the room and can also get absorbed in some really interesting and deep conversations, but I can very easily forget to think about my own needs – so I over eat, rather than recognising when I’m full and I stay out late, when actually I could do with an early night etc. Needless to say, these sub-types have a huge bearing on how we respond within our individual types.
Type 1 – The Perfectionist/The Improver/The Reformer
Enneagram Worldwide
As children, Type Ones tend to see the world as being pretty perfect and are ‘good children’. Their inner desire is to be able to play and enjoy life. But they begin to realise that life is not perfect. In fact the world is very imperfect, damaged, flawed and spoiled by all kinds of things over which they have no control. They have a need for things to be perfect. However, in their failed efforts to make happiness happen they develop a deep sense of anger (their root sin/stumbling stone) because their need is unmet. But they don’t want to project this to the rest of the world around them, because they are ‘good’. So they develop an ego projection to world that they are ‘reasonable’ – and this leads to rigid self-control. This then causes some pretty unhealthy behaviours, both for themselves and towards others, which are particularly hard to admit to and face up to. These include being self-absorbed, emotionally reactive, controlling, unhelpfully perfectionist, critical and actually deeply resentful of the world around them that isn’t the way it should be.
The invitation for all types is to face up to their deepest stumbling stones/sin and this is a really hard thing to do. It sounds brutal, but the invitation for the One is this: to admit that they are actually deeply rebellious and selfish. To stop their judging of others and to stop their unkind self-critique. If they do this, they make room in themselves for irrationality and messiness. When this happens it allows them walk into and receive the grace of an inherent sense of joy and lightness in simply ‘being’ and to find a real integrity between the inner experience and the outer expression. They come into a place of integration where they let go of the anger, so that it no longer controls them and find their inherent goodness allows them to experience life in its fullness and truth. When Ones step out of their ‘ego-structure’ and into ‘gift’ they become incredible leaders. They inspire and instil a sense of goodness. They make a difference in issues of social justice because they know that the world can and should be better than it is right now. They bring change to society through encouraging others to be their best selves and make fantastic coaches and communicators.
Type 2 – The Helper/The Giver/The Server
Enneagram Worldwide
As children, Type Twos deeply long to connect to others. They would struggle to admit it, but at the root of their problems is the reality that they struggled to get the attention they craved or felt like they deserved. They lack a sense of inner peace that they are deeply and unconditionally loved. So, in a bid to get noticed, they develop a need to be needed by others and start to believe that people will not be able to cope without them, which leads to their stumbling stone/root sin of pride. This leads to the development of their ego projection to the world that they are loving and helpful people. To others it seems like they are reaching out and connecting, always giving of themselves. But deep down this is what the Two craves – the acknowledgement that they are kind, helpful and giving of themselves. But what is really happening (and it’s hard for two to face up to this) is a need to dominate and control others with this attention, which they need in order to fill their inner void.
The invitation for a two then, is to admit to the negative feelings they have towards others (and themselves) and to allow their own needs to be important and to be met. In doing this, twos discover and receive the grace that the are deeply and inherently loved and accepted. Not for what they do, not for how they help, but simply for who they are. This allows them to stop being shaped by their need and become truly loving out of a place of knowing that they, themselves, are loved. In their best selves, they become full of strength, vitality and bring a gift of true mercy. They bring deep comfort and empathy to the people and communities around them. They are incredible ‘servant leaders’, no longer worried about getting the attention themselves but able to pour out their love for others, knowing that they are filled from a different source altogether.
Type 3 – The Achiever/The Performer
Enneagram Worldwide
As children, Type Threes realise that they are vulnerable and they begin to worry about what might happen to them, if people discovered what they were really like. So, through self-effort and self-creation, they become like a demi-god and create an ego projection to the world that they are outstanding. They develop the remarkable ability to play exactly the right part in whatever setting they encounter, because they have a deep need to be successful – but in doing so, they let go of their true self and so fall into their ‘sin’ of deceit. In fact, they can wear so many masks that it’s difficult for them to know their own true self. This leads to them seeking external validation to gain their sense of worth. However, what this leads to (over production, being over stressed, self-neglecting and disengaged from reality) is the exact opposite of what they crave.
The invitation for a Three therefore is to allow themselves to admit to their own anxiety and self-doubt. These self-made individuals are often racked with insecurity. When they stop and acknowledge this, they can relax into their own skin and stop needing to perform. For a three this is most often possible when they fail or when something happens which means they can’t perform for a while. When this happens, they can discover and receive the grace that being is enough – the place of true faith and they become grounded in belovedness. It doesn’t mean they stop achieving – it means that they learn to operate out of a sense of knowing who they truly are through an ‘internal’/deeper sense of affirmation, rather than the need for this to come externally. Healed Threes recognise failure as a gift. They are able to let go of the need to excel to win and become simply excellent! They make wonderful leaders and bring a sense of drive, and achievement to the teams they work in and with. Threes don’t just see the vision, they deliver it.
Type Four – The Romantic/The Individualist
Enneagram Worldwide
As children, Type Fours have a sense of lack or real/perceived suffering. They carry a deep sense of being somehow tragically defective in some way and ‘cast out’ or like they are a misfit, who noone can quite understand and so they develop a kind of longing to be rescued. This creates a sense of comparison and others and leads them to their root sin/stumbling stone of ‘envy‘. So they create an ego projection to the world around them that they are sensitive, which pulls people towards them because they are ‘mysterious’ and feel things deeply. They have a need to be special. But this can lead to them being experienced as emotionally reactive and unpredictable. And this is used by the four (unconsciously) to control and manipulate relationships.
The invitation for the Four then is to admit to themselves and others that they are judgemental, envious and critical of others. They then have to risk letting go of their inner identity building in opposition to others and instead receive, in place of their felt sense of deficiency, the grace of an identity of ‘inherent and fundamental goodness’. This integrates with a sweetness and generosity of Spirit and allows the Four to bring an incredibly gift of beauty, artistry and creativity to the world around them. Fours make the world beautiful. They carry incredible creativity and wonder. They are incredibly emotionally perceptive and intelligent and pick up on ‘atmospheres’ and under currents. They are true empaths – sensitive, loving and at their best able to hold space for others to do their own work, without taking it on themselves.
Type 5 – The Observer/The Investigator
Enneagram Worldwide
As children, Type Fives have a desire to assert themselves and take control of their world. But they find that the world fails to satisfy their inner emptiness. So they disengage and become more withdrawn (it’s quite rare though not impossible to be a Five AND an Extrovert!). Fives withdraw into their minds, because that is where it feels safe and they stumble over their root sin/stumbling stone of Avarice/Greed. This can be greed for ideas, but can be material accumulation also – Mr Microsoft is a classic Type Five. Fives develop a deep need to perceive. It is through their superior knowledge base that they can control their surroundings and gain an inner sense of superiority. So their ego-projection to the world is that they are perceptive and wise. This leads to some classic behavioural traits of withdrawing into their minds to ‘figure things out’. But this can lead to them being quite absent, distracted and have a hyperactivity of their mind – unable to ‘get out of their head’. One thing that can happen to a Five is that because they spend so much time in their head, they forget to listen to what their body needs because to them, what really matters is their mind, their thoughts, their ideas.
The invitation to a Five then is to admit to themselves and others that they use knowledge to dominate and undermine others. They then need to risk getting in touch with their heart and allow themselves to feel things more deeply. When they do this, they allow themselves to stop being so standoffish, to receive the grace of real self-confidence and find they can get involved in community and society rather than observing it from their ivory tower, firing sarcasm from a safe distance. When this happens they can also integrate with a deep sense of joy and lightness of being, bringing much more earthed wisdom and understanding into the world around them. Fives bring incredible wisdom and understanding to society. They are well read, able to dig deeply into complex ideas and make it available to the rest of us. Fives care about detail and this is important. They also bring a reality check with a sense of humility to problem solving.
Type 6 – The Loyal Sceptic/The Patriot/The Loyalist
Enneagram Worldwide
Most Enneagram teachers believe that Type 6 is the most common Type – according to Richard Rohr, perhaps up to half the population might be Type Sixes. As children, sixes have a deep desire to be comfortable and for nothing to need to trouble or worry them. But they realise that the world is not altogether safe – it is random. This leads to a deep and existential sense of fear, which becomes their stumbling stone/root sin. As a result they develop an anxious alertness and believe in the idea of survival of the fittest. They therefore develop an ego projection which is that they are reliable, they are loyal and also sceptical. This leads to them seeking security externally. They can come across as true patriots – often looking for a leader who will make them feel safe – perhaps this is why in a time of uncertainty, political rhetoric around securing our borders and making our nation-states great again (Brexit/USA narrative) lands with so many voters. As a result of wanting to preserve this image of obedience and loyalty, Type-Sixes can easily become workaholic and expedient through are also quite image conscious because they worry a lot about what others think of them.
The invitation for a Six then is admit to themselves and others their deep need for security and comfort. Once they have done this, they need to risk quietening their minds, their anxious ruminations, their worries and their constant catastrophising of the future and instead learn to be still. When they do this, they will learn to receive the grace to be relaxed and trust in ‘Being’, knowing their inherent value. In this way and from this place of mindfulness, heartfulness and being present in the moment, they become truly loyal, faithful friends and can accomplish many great things with a sense of deep peace. Sixes make brilliant strategists. They see things very holistically. They consider the possible humps and hurdles on the road in front and are able to plan to mitigate these issues ahead of time. They ask good questions, see things from lots of different angles and perspectives and bring a much needed sense of realism to their work.
Type 7 – The Enthusiast/The Epicure
Enneagram Worldwide
OK – full disclosure – this is my ego-structure!
As children, Sevens develop a sense of lack – that there might not be enough and feel overwhelmed by a build-up of issues. They respond to a sense that the world, or those around them have failed to make them feel content or safe. So, in search of ‘paradise lost’, they escape their sense of or fear of deprivation by drowning out any pain with pleasure. This leads to their root sin of gluttony – of food, or anything really – a false comfort, so they don’t have to face the reality of the pain they are feeling deep down. They develop a deep need to avoid pain, almost at any cost. So they project to the world that they are enthusiastic. Sevens can be huge fun to be around. However, much of this is ‘fake joy’ based in anticipatory energy of the next brilliant thing that’s about to happen rather than being present in the moment. As a result Sevens can become highly controlling of themselves and their environment in order to suppress the truth of what they are feeling. They want it to be fun! But this can be exhausting…..
The invitation for the Seven, therefore, is to admit to themselves and others that they really are overwhelmed and face the reality of the pain they are running away from. When they do this they recognise their deep dissatisfaction with life as it is and can learn the grace of contentment. When this happens they can receive the grace of discovering simplicity and a restored ability to focus. When they integrate this with a sense of things being OK just as they are without a constant need for more, then they can bring real, deep and lasting joy to the community and world around them. Sevens bring real deep, sober joy and gratitude to the world. They are enthusiastic and effusive, never lacking in vision or hope. Life is to be celebrated and Sevens love to party. They have an ability to assimilate lots of different perspectives and communicate in a way that galvanises people into action.
Type 8 – The Challenger/The Protector/The Leader
Enneagram Worldwide
As children Eights have a deep desire to be held and loved, but they experience a real or perceived failure of others to love them as they need. This leads to them feeling let down. So they become determined to never be needy of dependent on anyone else ever again. They live to believe that they are in control and if they need something, they will get it for themselves. This causes them to stumble into their root sin of lust. Lust for power, lust for control, lust to dominate others. And so they project an ego to the world that they are strong. And as a result they have a need to be against. Against the expected status quo. Against the flow. Against the societal norms. This leads to assertive behaviours to demonstrate their strength and fierce ability to cope. But in doing so they become completely detached from their own needs. This can drive others away, and can be experienced as bullying – the exact opposite of what Eights actually crave, which is relational intimacy.
Difficult though it may be, the invitation for the Eight, therefore, is to let their guard down. To admit to themselves and others that they have weaknesses and unmet needs. And if they can risk openness or vulnerability with others then they will receive the grace of the experience of being truly loved. When they integrate this with deep clarity, insight and perception they bring true strength to the world and their desire for social justice, rather than burning them out, can come to the fore as a true gift. Healed eights make brilliant leaders. they look after their teams They carry a deep sense of social justice and they are not afraid to upset the apple cart to achieve this. They both challenge and inspire people to do the stuff that matters and live their best life.
Type 9 – The Peacemaker/The Mediator
Enneagram Worldwide
As children, Nines have a sense that they want to be someone special and get noticed. However, they somehow come to believe that this will only happen if they make it happen by themselves. Not so keen on this idea, they fall over their stumbling stone or into their root sin of sloth or laziness. As a result, they become self-forgetting, zone out from the world, function on autopilot and tune out from the depths of life and project their ego onto the world that they are peaceful, easy-going and will fit in with anything. In so doing they lose themselves. But as they have developed a need to avoid, they don’t mind too much, as long as they feel comfortable. This leads to them becoming both anxious and passive, but when challenged can aggressively defend their comfort zone.
The invitation for the Nine, therefore is to admit to themselves and others that they actually do want and need attention. When they do this, they risk experiencing intensity and energy – but when they do it enables them to receive the grace to discover their inherent value. When they integrate this with real faith and courage, they can be present to the world around them and become true peacemakers and mediators – a much needed gift in our communities right now. When present to the world around them, Nines can bring incredible energy and purpose. They are able to hold the space for deeply uncomfortable and difficult discord and use their skill to bring reconciliation.
So many of our physical and mental health problems are amplified/worsened/affected by our personality traits. I hope these brief insights have been helpful and create a way of thinking about how your own personality might be affecting they way you view your won body, your own self-worth and how you are creating a story to the world about yourself that might need undoing. When we do our internal work and allow ourselves to admit how much it is actually costing us to keep on living in the way of the ego, we can learn to let go and receive the grace to become our true and best selves. Perhaps when we do this, some of our battles stop being about what we can control or what we are running away from and we can learn to live more presently in the world, awake to ourselves and able to make choices worthy of who we really are.
Last week the Chief Medical Officer, Professor Chris Whitty, came up to Lancashire. He spent the morning in Blackpool and then came over to see us in Morecambe Bay for the afternoon. It was an absolute pleasure to meet him and to welcome him here. He came to listen – the mark a genuinely kind and caring leader. More importantly he came to listen to people who live in these Northern Coastal Communities, to really hear what life is like and to allow that to impact his thinking and he prepares to develop further strategy on tackling poverty and health inequalities. As an epidemiologist, he is grounded in data and understands the issues at hand. What I really valued was his humanity and humility as he listened to the stories of people who live and work here.
Last year, the Home Secretary, Pritti Patel also visited Morecambe Bay. She came to Barrow-in-Furness and spent some time at The Well, a CIC which works with people in recovery from addiction and of which I am a Director. In an interview afterwards, she was asked about the impact of Austerity and the reality of poverty in communities like ours (4 in 10 children in Barrow grow up in poverty). Her answer was that poverty is not the (sole) responsibility of government. I put sole in brackets, because she tried to insinuate that the role of central government in tackling poverty that exists in local areas is very minimal compared to the responsibility of local government (who have had their funding massively cut by central government in the last 10 years), local schools, local public services and local businesses. I’ve really wrestled with what she said since that time because she’s not altogether wrong! But nor is she right! Of course Central Government has a huge role to play in tackling poverty. It’s undeniable that national policy, economic strategy, including taxation, land ownership and business development all have massive implications. But poverty doesn’t only exist because of Central Government. Health Inequalities do not just exist because of Central Government. I am not for one minute, negating or diminishing their role, but we do have to all ask ourselves why we see and tolerate such inequality and what we can all do to change this narrative. Because as Michael Marmot reminds us so powerfully in his book ‘The Health Gap’ – none of this is inevitable and it certainly doesn’t have to continue. Marmot holds that “if you want to understand why health is distributed the way it is, you have to understand society.” So if we want to understand society, then as Prof Bev Skeggs (Professor of Sociology at Lancaster University) so eloquently says: “Society is shaped by our values and what we value“.
If we are serious about ‘levelling up’, ‘resetting’ and tackling age old health inequalities then we have to understand that this is both complex, but also entirely possible and need not take 100 years! As Marmot says in his amazing book ‘The Health Gap’ – essential reading for anyone who cares about this issue – we must do something and we must do it now! Marmot’s research proves that health inequalities are not a footnote to the health problems we face, they are the major health problem. We can actually make significant and measurable differences in a short space of time – so why aren’t we doing more? In the rest of this blog I hope to look at how we can make a real difference to poverty and health inequalities in our communities. We all have a part to play, no matter who we are. This is absolutely an issue for central and local government, but it is also an issue for society as a whole in all its facets.
Prof Imogen Tyler has written a phenomenal book called ‘Stigma: The Machinery of Inequality’. It is, in my opinion, the most important book published this year (I know that sounds like an overstatement, but it isn’t!). I believe this must be our starting point when we talk about poverty and health inequality. If we don’t understand how we have all subconsciously and/or overtly accepted a narrative that ‘the poor are feckless and lazy and could just pull themselves up by their boot straps if they wanted to, because we all have the same opportunities,’ then we are blind to the reality of the stigma that surrounds poverty and how it is weaponised to maintain the status quo. The thing is – it’s not just the government who have used this narrative – it’s part of British culture. So many of our comedy programmes ridicule and scapegoat the poorest in our society – The Harry Enfield Show (‘The Slobs’), and Little Britain (Vicky Pollard) to name just two. think of how many reality TV shows, like ‘Benefits Street’ have reinforced the stereotypes. Our national press continue to bombard us with very particular perspectives on ‘benefits scroungers‘ and ‘migrant swarms‘ and we read it, we drink it in, and whether we like it or not, it embeds itself as a way of thinking in our minds. That’s how propaganda works. It creates a corporate mindset by ‘othering’ our fellow human beings and pitting us against one another, rather than bringing us together to collaboratively find solutions in a way that works for everyone. It takes significant and sustained effort to do our own internal work around stigma, racism, white privilege, sexism and toxic masculinity. But if we want to build a society shaped by our values and what we really value then whoever we are – this is where we must begin. Our first work is to demolish the strongholds in our minds, challenge our unconscious biases and undo our ‘go to’ narratives, replacing them with deeper and better truths about the innate value in every human life. We must be determined to create the kind of language which reflects this because language gives substance to our thoughts and beliefs. This important work needs to weave its way through every part of our education system. This will take effect in shifting the corporate mindset through the way we teach history in our schools, for example, with a more honest appraisal of the negative effects of colonialism, or indeed how the feudal system continues to dominate the price of land and the unaffordability of good quality housing. We need to equip the rising generation with the tools they will need to undo the damaging ideologies of stigma and find solutions to the issues they are facing around social justice and climate change.
Imogen draws on the work of The Poverty Truth Commission, here in Morecambe Bay and in other places to highlight ways in which we can break down stigma, build friendships and create a kinder society. The Poverty Truth Commission gives us a real insight not only into how we break down stigma, but how the building of friendships across the dividing walls in our society creates a new political space from which we can create ‘the good life’ together. Our political systems have become far too removed from every day life and we need a radical shift from disengagement to much wider participation in community life and decision making. There are so many voices calling for this from all sides of the political spectrum. We so badly need to break out of our entrenched twitter-siloed positions and learn to curate the space for a more collaborative and co-operative form of political and economic conversation and prioritisation. It is, in my view, impossible to think about breaking down health inequalities without involving those who experience them most severely to be a part of finding the solutions. For further reading on this: Radical Help by Hilary Cottam, Rekindling Democracy by Cormac Russell and Greed is Dead: Politics After Individualism by Paul Collier and John Kay are all vital texts. This requires a much more local, devolved, participatory kind of politics – the kind of thing made possible through initiatives like ‘The Art of Hosting’, ‘Citizens Jurys’ and ‘People’s Assemblies’ underpinned by principles of love and kindness. In this way we can create much more realistic ‘deals’ (like the one in Wigan) between public sector organisations and people in our communities. This might all sound a bit wishy washy, but as Marmot demonstrates, “the lower people are in the socio-economic hierarchy, the less control people have over their lives.’ He argues that “tackling disempowerment is crucial for improving health and improving health equity” This is where the circular arguments about absolute or relative poverty are missing the point. When Philip Hammond stated as Chancellor of the Exchequer that he ‘doesn’t see poverty in the UK‘ – he was talking about absolute poverty and implying it isn’t an issue in the UK. He’s profoundly wrong. Economist Amartya Sen helps us understand this: “Relative inequality with respect to income translates into absolute inequality in capabilities: your freedom to be and do. It is not only how much money you have that matters for your health, but what you can do with what you have; which in turn, will be influenced by where you are.” Marmot argues that this means people in this position cannot participate in society with dignity. It is this active participation in ones own life and the life of the community around you, coupled with a sense that you can be part of the change that needs to happen which underpins the strap line for the poverty truth commission. “Nothing about us, without us, is for us.” If we want to tackle poverty and health inequalities in our society we have to radically include those who are currently most marginalised to be part of the change with us. We’re not trying to fix them. Together, we are trying to untangle the injustice that allows this kind of staggering inequality to continue.
The NHS is currently exploring its own role in tackling poverty and health inequalities. As the biggest employer in the country it has the opportunity to make a massive difference as an Anchor Institution, setting a good example and creating a network, both locally and nationally for other partners to collaborate with. Along with other local employers it can make a vast difference through positive employment schemes for people from poorer communities, paying a living wage, procuring locally and developing apprenticeship schemes, to name just a few ideas. We have developed a charter in Lancashire and South Cumbria, which we hope will be nationally available soon. I’ve previously written on the role of Primary Care Networks (PCNs) and how taking a ‘radical help’ approach with our communities could make a real difference at a local level. PCNs have a particular role in Population Health Management. This approach that we are focusing on across Lancashire and South Cumbria uses the best in data science and enables health teams to focus in on the areas of greatest need, working with those communities to bring about change through co-creation. If the NHS is really serious about ‘levelling up’, however, one thing which must be explored is the national funding formula. If we’re serious about Population Health, we must be much more comfortable with allocating resources according to Indices of Multiple Deprivation. We must also change what we measure and ensure that Key Performance Indicators and clinical funding streams are much more aligned to this entire agenda. Incentives do change behaviour and we need to make sure that we’re getting them right, whilst permissioning PCNs, in particular, to have a change in focus. We need to make it more attractive to work in areas of higher complexity and create more sustainable models of care. It is my belief that without a Health Inequalities lead at the top table of NHS England and Improvement, the right level of accountability and prioritisation simply won’t be there. It won’t be enough just to have someone accountable in each system, vital though this is. Integrated Care Systems must take an evidence-based approach and recognise what a profound difference they can make in a short space of time. The drivers in the system must be wedded to this way of working. The NHS must stop spending such a colossal amount of money tinkering around the edges of helping people to live a bit longer and get deep into the game of tackling the vast and ongoing health inequalities in our society. It must use it’s powerful voice to continually challenge policies which make this worse and actively campaign to make society more equitable. Marmot and The King’s Fund have already detailed so much that the NHS can do. Olivia Butterworth and Sara Bordoley and their teams are doing some great things. We need more of it! It’s time to act!
The issue of land and the lack of affordable housing has a huge effect on people being locked in cycles of poverty and creates massive health inequalities. Central Government has a huge role in sorting this out, but increased devolution may make it become easier with increased public participation in the daily politics of life. Most of the way our land is distributed and inflated was designed in the 11th Century and through the Middle Ages. Alistair Parvin has written the most phenomenal piece on this issue and it deserves time to be read and digested. He makes a very tight case as to why we find ourselves in the situation we are in, but encouragingly he comes up with some really possible, pragmatic and solutions-focused ideas about how we can solve this, if we want to. Of course there are many vested interested and people in positions of significant power, who would resist such an approach, but we must not let that stop us having some grown-up conversations about this. Parvin accepts that it would take a government with extraordinary vision and bravery to do what is really needed and offers some really helpful pragmatic smaller steps that would get us in the right direction.
I am not going to copy and paste his paper here, but I hope this whet’s your appetite enough to seriously engage in the possibilities. We can’t keep passing this ball to future generations. We have a once in a lifetime opportunity to reset our economy and in this time of ‘jubilee‘ we need to grasp this nettle if we are serious about creating a society that truly works for everyone. Mariana Mazzucato, Kate Raworth, Katherine Trebeck and Carlota Perez are just some of the brilliant people creating the kind of economic and technological frameworks we need. It’s time to build an economy of hope, shaped by our values and focusing on what we value. We know that the UK population would like us to place health and wellbeing at the heart of the UK economy instead of GDP – this is a massive shift and one that we must hold onto. This priority along with the creation of more social co-operatives, new local/community banks and credit unions would all help us to create a fairer economy that really works for the people.
So, we all have a role to play. As individuals, in our communities, through our work and via a more engaged, participatory, devolved, democracy, we need to deal with stigma and ‘wicked issues’, be determined to be more switched on, truly engaged and find together some pragmatic solutions fit for the 21st century. Disengagement is not an option. Let us not miss this moment. We can and we must do something. As Michael Marmot says in the final sentence of ‘The Health Gap’: “Do something. Do it more. Do it better.”
Prof Steve Peters, renowned psychiatrist, (particularly for his work with Sports teams) has written a brilliant book called ‘The Chimp Paradox’, which I regularly recommend to my patients. It’s well worth the read and full of helpful and practical tools to enable effective mindset and behaviour change. In it, he teaches about the 3 main parts of the brain when it comes to our habitual behaviours – what he calls The Chimp (Limbic System – where we make our immediate responses – based on our feelings and impressions), The Computer (the parietal cortex, which stores our automatic programmes and responses based on our beliefs and experiences) and The Human (the frontal cortex, where we do our thinking and make more conscious choices based on fact, truth and evidence, usually from a place of compassion and empathy). Many times we find ourselves acting in ways which are simply responses of our chimp brain – we’re not being guided by conscious choices or values, or even if we want to, we can’t seem to overcome the strength of our chimp. The problem is that our chimp is 5x faster than our human brain. And if we also have ingrained trauma-based responses to certain situations, when we are triggered (e.g. when we feel scared or lonely or whatever), our chimp gets ready to act, checks its facts with the computer which agrees that this is how it should/would usually respond and a bar of chocolate later……. Same old cycle, same old shame…..
So how can we change these patterns? Well, we need to feed our computer brain some new messages, so that when the chimp starts acting out and checks in with the computer, the computer no longer agrees with that old way of reacting, puts a pause on the chimp and allows the human brain to kick in with more positive choices. This happens, by consciously renewing your mind by feeding your mind your core truths and values. When you fill your mind with what you know to be true and the values you want to live by, you begin to make different choices. Your computer begins to store new and different information and therefore when your Chimp begins to act out, it will check in with your computer and find that the automatic affirmation of a learned behaviour can begin to change. This has huge implications in how we think about ‘taking responsibility’ and managing our own behavioural choices. I also think it has a wider application to our corporate mindsets and behaviours which cause us to continue acting in certain ways in society (which I will come onto later).
So, I have some core truths and core values which my lovely wife has painted on a board in my office. I have them written in my notebook, and (now less then I used to – to begin with it was at least twice a day) I remind myself of them regularly.
Here are the Truths that I live by:
1) I am unconditionally loved by the community of God (who unconditionally loves everyone and in whom we live, move and have our being), my wife and a bunch of other people
2) I am seen and accepted for who I am
3) Being a husband and a father are more important than any status I can ever achieve in work
4) It’s OK to make mistakes – in fact, failure is a gift
5) I can’t do everything – limits are important and so are teams!
6) Life is not always easy and happy, in fact it is unfair and really sucks at times – pain is part of the journey
7) People may not always deserve love and may not be easy to love, but you can still choose to love them – even your enemy
8) Forgiveness is a choice and it sets you and the other person free
Here are my Values:
Love people unconditionally
Walk with humility and integrity
Listen with kind eyes
Seek first to understand
Encourage and Forgive others and yourself
Act gently
Live generously with extravagant hospitality
Be open, honest and vulnerable
Leak joy
Release healing and hope
Walk in peace
Be faithful
Speak truth with compassion
Embrace pain
If you don’t know what is true and you don’t know what your values are, you cannot line up your behaviours to match them. If every time I experience pain, in whatever form that may take, I need to find comfort in a self-destructive behaviour, I have lost sight of my truths that I am unconditionally loved, that life sucks sometimes and have let go of my value to embrace pain. However, if I accept that I mess up sometimes. then I can forgive myself, and get back on track. It doesn’t have to mean a downwards slide. This is how change happens – slowly, but encouragingly as I learn to focus on who I am becoming, rather than believing I will never break out of unhelpful habits.
In her brilliant book, ‘The Value of Everything’ in which she talks about an Economics of Hope (how good is that?!), Mariana Mazzucato applies some of this thinking into the realm of how we build a society based on our values. What if we broke out of some of our self-defeating societal norms and built our economy from the best of our compassionate values? I wonder how many of our corporate chimp-computer agreed behaviours might change if we really examined what we value when it comes to the way we build society, through our economics and politics. So much of the time we are sleep walking with our eyes wide shut to the mindsets we unconsciously imbibe, which shape our corporate behaviours and choices. How often do we examine our core values or the truths that we live by? It takes determined effort to demolish strongholds set up in our minds and replace them with a renewed set of values with which we can build a more loving and kinder world. What would this mean for health inequalities, poverty, and who or what we might choose to prioritise? Without this work, however, we will continue to behave in ways which tolerate huge social injustice and climate destruction. But things do not have to remain as they are. We can change! Hold onto hope! In this apocalyptic moment, in which we are seeing the realities behind the facades more clearly than for many years, it remains time to rest, reflect, reimagine and reset.
Test and Trace is currently an absolute shambolic mess and there’s no point pretending otherwise. Over the weekend, a mum I know of in Morecambe was told to drive over 130 miles to have her children tested, only to find that the centre was shut when she got there! I know of another woman in Skipton (that’s in North Yorkshire, if you’re unsure), being sent to Northern Ireland! This cannot go on. It’s beyond ridiculous! It also massively undermines the idea of levelling up, because families who can’t afford to travel further then have to keep their children out of school for longer, causing further disadvantage to their learning opportunities. Imagine having a fever, feeling unwell and then being asked to drive a long distance to get a test, which should be available in your vicinity. It’s unsafe. It’s also unfair to blame people for booking tests unnecessarily when a) people are only able to get a test if the people employed by Serco allow them to have one, b) children can’t go back into school, once sent home until they are proven ‘negative’ and c) the Prime Minister has promised testing to pretty much everyone via his ‘Moonshot’ approach.
It’s vital, as we enter the winter months, to get this right. Our ability to provide safe staffing levels across the NHS and enable schools to function properly genuinely depends on it. Last week at the NHS Assembly we debated the issue and a possible way forward. The contract issued to Serco is clearly not delivering what is needed, and so it’s time to take an honest appraisal of where we are and how we’re going to fix this. I know the Assembly will be writing in an official capacity to Dido Harding, who is currently in charge of the programme. In the mean time, here are my thoughts about what needs to happen now.
It’s time to value the brilliant local public health leadership we have in place across the UK and ensure these leaders are supported to lead this work by providing timely data. After investing in the training and expertise of our Directors of Public Health, why on earth at a moment for which they have been trained to provide leadership are we circumnavigating them and making it so much harder for them to do their jobs? It would be worth an apology for not trusting them to do this in the first place and to own up that ‘Serco Test and Trace’ (not ‘NHS Test and Trace’) has failed in its task.
We must ensure that local councils and Directors of Public Health have the resources necessary to lead the local test and trace approach and ensure they have the necessary powers to intervene where needed.
The whole system must work – so we need to create more capacity in the laboratories across the UK to turn around results in a timely fashion.
It’s vital that we engage regularly with local communities of many different kinds and their leaders to ensure they understand where things are up to, how we can work together to keep people safe and debunk any myths that are developing, whilst holding space for the uncertainty of the moment.
Therefore we need clear, comprehensible messages to the public – we need to empower/permission local teams to lead on this messaging in a way that makes sense for their communities without constantly needing to check back with the centre. This comes down to trust.
The NHS and Local/National Government need to become much more comfortable with using different communication channels like WhatsApp – and for young people Instagram, YouTube and Tik Tok – because this is what young people are using now to the exclusion of nearly everything else…..if we have unclear messaging and then don’t even use the platforms that young people are using, we have no right to scapegoat them (which is terrible practice anyway!).
It’s really important that testing capacity is available rapidly and flexibly in areas with outbreaks. With the R number rising as it is and the current farce around availability of local tests, we simply can’t afford for this to continue.
We must recognise the value of and therefore ensure early intervention and action ,rather than delaying decisions. This has been highlighted by Sir Jeremy Farrar, CEO of The Wellcome Trust and member of SAGE in some current learning form Marseilles, where the hospitals are back at the point of saturation.
I’m not sure how or why it was decided that Serco should run this show in the first place. However it’s clearly not working. It’s time to make brave decisions. It’s time to get this local and focused. It’s time to get this right. Our lives may actually depend on it.
Yesterday, I tweeted that I think Dido Harding, the Chair of NHS Improvement and newly appointed head of the newly established National Institute for Public Protection (NIPP), which is to replace Public Health England (PHE), is a good leader. I say this, having met her and few times, through the NHS Assembly and her genuinely humble desire to listen and treat people with kindness. It caused quite an interesting discussion and there has been widespread criticism of her appointment.
Last week I did my yearly updates of the mandatory online training required in the NHS. Part of this included my ‘fraud awareness’ and this focuses, particularly on the Nolan principles – an ethical framework under which we are required to work. If these principles are not followed, people can quite rightly lose their jobs and even be sent to prison. The principles apply to all people who work in public life, not just the NHS and are as follows:
1. Selflessness
Holders of public office should take decisions solely in terms of the public interest.
2. Integrity
Holders of public office must avoid placing themselves under any obligation to people or organisations that might try inappropriately to influence them in their work. They should not act or take decisions in order to gain financial or other material benefits for themselves, their family, or their friends. They must declare and resolve any interests and relationships.
3. Objectivity
Holders of public office must act and take decisions impartially, fairly and on merit, using the best evidence and without discrimination or bias.
4. Accountability
Holders of public office are accountable for their decisions and actions to the public and must submit themselves to the scrutiny necessary to ensure this.
5. Openness
Holders of public office should act and take decisions in an open and transparent manner. Information should not be withheld from the public unless there are clear and lawful reasons for so doing.
6. Honesty
Holders of public office should be truthful.
7. Leadership
Holders of public office should exhibit these principles in their own behaviour. They should actively promote and robustly support the principles and be willing to challenge poor behaviour wherever it occurs.
from The Guardian
The decision to disband Public Health England, (which is recognised internationally as a world leader in the realm of Public Health) and the appointment of Dido Harding into her new role (even though I do really like and respect her) are not aligned with the Nolan principles and I believe therefore that the Secretary of State for Health and Social Care, Matt Hancock has some serious questions to answer, which are absolutely in the public interest. Each of those questions should be framed around the Nolan principles and are a part of the accountability required in such a momentous decision. It’s not that Dido Harding (who called for more integrity in NHS leadership) is necessarily the wrong person (although many feel that she is). It’s the way the appointment was made that makes everything so murky and this is a great shame.
Public Health England must not be used as a scapegoat in the forthcoming independent enquiry into the UK’s response to Covid-19. We must also better understand where and how its other vital functions will be performed. As Jeanelle de Gruchy, President of the Association of Directors of Public Health, has so eloquently argued, the NHS is not currently set up to do this work. There is the potential that the newly established Integrated Care Systems (ICS’) across England, which bring together public sector partners, including the NHS and local government could hold the responsibility, but this would need to be funded adequately and appropriately AND would require a legal framework, which is currently lacking. We simply cannot afford to lose the vital functions of prevention, child health and other huge programmes previously co-ordinated by PHE. With further financial issues ahead for local government, the idea that public health prevention will remain a priority, when we have already seen the roll back of this since 2010 is unrealistic. If this happens, rather than ‘levelling up’, the great promise of the Prime-minister, Boris Johnson, we will see a worsening health inequality gap and those in our poorest communities struggling even more.
We need urgent answers to urgent questions. But more than this, we need a government who are willing to act with integrity, openness and through the proper mechanisms of parliament. Announcing major changes to the functions of public sector organisations through the press and the refusal to follow good processes in redesign are seriously unwise and unfair. Trust in this government is waning and they could do a great deal more to rebuild that trust, if they care to do so. The loss of Public Health England matters, not only because it does such incredibly important work beyond public protection, but because of the manner in which it was disbanded and what this means about how government is functioning.
When Matt Hancock made his speech about his new NIPP yesterday, he finished his Q&A session by talking about the “Holy Trinity” of Academia, Government and the Private Sector. I see very little that is holy about this triad, especially if the Nolan principles are flouted. The Trinity I know is full of love and truth…..I wonder what the consequences of this clear ideology will have on the future of the NHS. I fear the answer is not in the public interest.
In my last blog I looked at the complexity that surrounds the issue of obesity in our society. We have become far too focused on the individual and personal choice, whilst clouding the whole issue in shame and blame through stigmatisation. My hope is that we can talk about obesity with humility and compassion and re-frame the conversation from the all too often over-simplified position of ‘calories-in-calories-out’. Let’s be really clear as we begin to focus on what we can do as individuals, that we do not all start on a level playing field. We have different genetics, different sexes, different body types, different ethnicities, grew up in different environments, have differing belief systems and different personality types. We are different and this should be celebrated! So, this cannot be a game of comparisons. Tough though it may be for me to accept, I am never going to look like Joe Wicks! When I started to write this blog piece on how we might think about obesity as individuals and communities (given all the other complicated factors which make living well in an obesogenic environment so much harder), I thought that I would be able to write it fairly easily. However, I’m discovering that it could easily turn into a book! And so, I’m going to continue this a mini-series and write several more posts, partly so they are not too long and partly, so that I can explore the issues in more depth. The series does not aim to be the answer to every practical question about obesity, weight loss or positive body image, but I hope that it will be really helpful in setting out a way of thinking about the issues affecting us. I will look at some of the deeper causes and then some possible ways to find ways forward.
The Impact of Trauma and Adverse Childhood Experiences
I think we have to start here.
In the 1980s, Dr Vincent Felitti, Director of Preventative Medicine at the Kaiser Permanente Health System in San Diego, California, began to discover something troubling in his weight-loss clinics: there was a very high drop out rate and he couldn’t understand why. What we went on to discover, in conjunction with Dr Robert Anda, over the following 15 years was that around 50% of people in his clinics had suffered from a significant number of ‘Adverse Childhood Experiences’. Initially his patients would do well and lose weight and then stop attending and put their weight back on.Something I think we see again and again in the ‘diet world’.
Further studies across the USA and UK have shows that 50% of us have been through at least one ACE and around 10% of us have been through at least 4 of them. Trauma, especially in our early years, but actually at any time, can have a profound effect on our lives. The eminent Professor of Psychiatry, Bessel Van der Kolk, writes in his book ‘The Body Keeps The Score‘ about what changes take place in our brains, our genes and our subsequent coping mechanisms and behaviours as a result. The issue for many of us, who are ‘overweight’ is not that there is something wrong with us, but rather that something happened to us which has deeply impacted us ever since. My friend Lesley, an incredibly brave woman, whom I really admire, puts it this way:
“I wasn’t loved or nurtured as a child – I was abused. Sadistically. In every way. Although to the outside world we were a model family. I craved love and substituted it with food. I believe ACEs are a huge factor in obesity. In seeking comfort in food, I developed an emotional relationship with food. Rewards, celebrations, socialising, commiserating – we are all guilty of using food in these ways to a greater or lesser degree. Crack ACEs and I think we’d go a long way to tackling obesity and other ‘dependency’ type issues.“
(If you are familiar with this blog, you will know that I have blogged several times about what ACEs are and why they can have such a profound effect on our lives. There is also a link to a book I have co-authored on this subject here, – we have a new one coming out soon!). If you prefer podcasts, we have done one here.
For those of us who work in clinical settings, giving someone the chance to tell their story, rather than just referring them through to some new service or other can have a much more healing effect than we realise and might significantly change the next steps the person in front of us chooses to take on their journey. Giving a bit of extra time, to listen with kind eyes and to understand someone’s experiences can make all the difference in bringing real and lasting change.
Although not all of us who are overweight or obese have been through a terrible experience or trauma – it is true for many of us. Recognising the hard reality of trauma in our society and how rife it is, even within ‘model families’ helps us realise again the complex relationship we can develop with food and the resulting issues we can have with our weight. So firstly, let’s have some compassion in how we view ourselves and others, let’s not make assumptions about what people are like or what they may or may not have been through, because we don’t know their stories. Let’s also be committed to being trauma informed and a) help create the kind of society in which we see an end to as many ACEs as possible, whilst b) putting more protective factors in place to help children who are going through them and c) enable each other to get healed from the traumas we have experienced, without judgement. There are many things which can help us heal from trauma – the most important step is breaking the silence and the shame by telling someone we love and trust the truth about our story. Simply sharing the burden, being heard and validated is in and of itself deeply healing. Particular talking and psychological therapies like EMDR, family systems therapy and trauma-focused CBT are a helpful next step, alongside various physical therapies, which help us learn to live in our bodies without having to be defined by the traumas we have experienced. These can be available in certain NHS mental health teams, through various charities and private therapists.

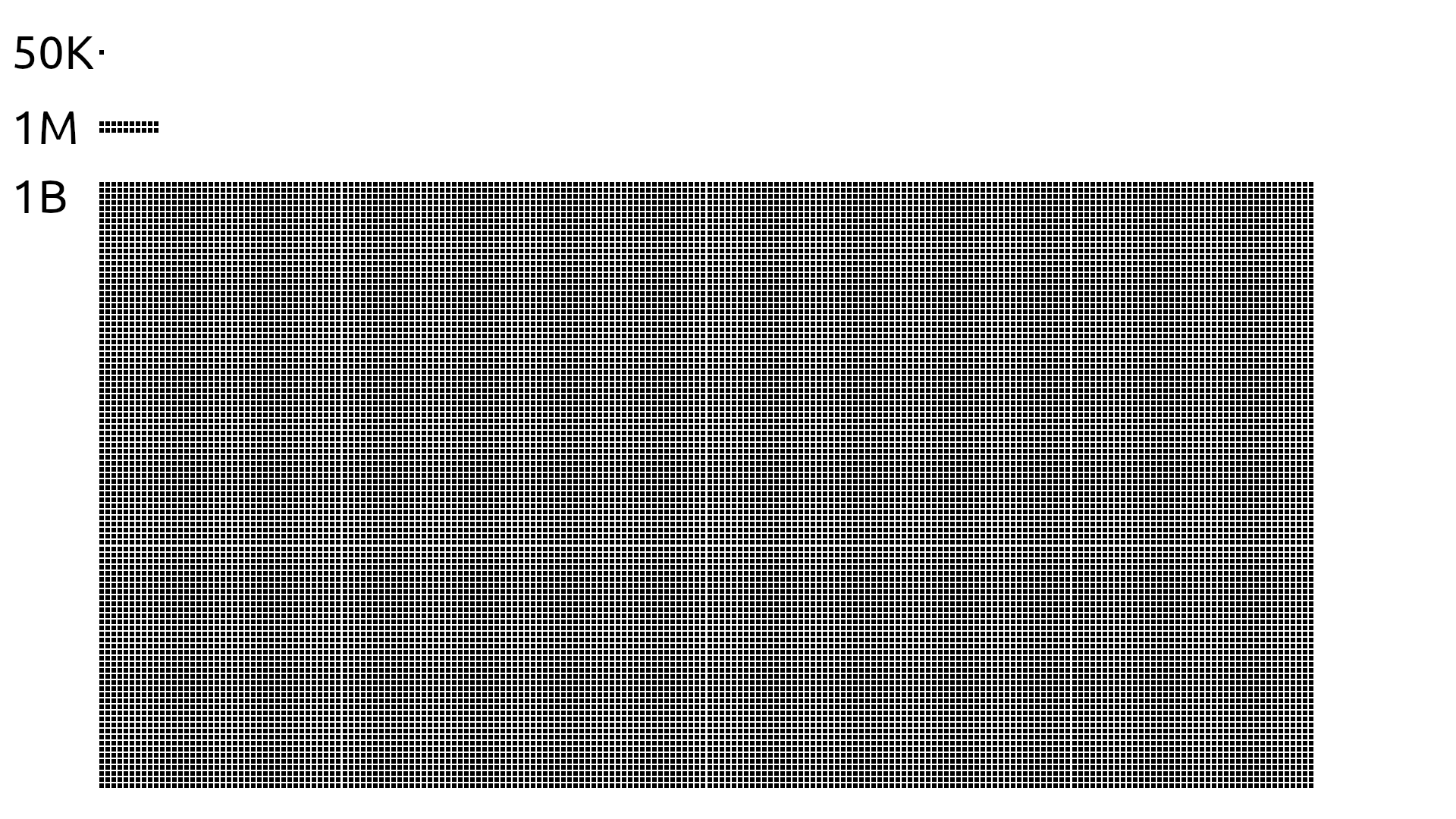 The things is that most of us find it hard to comprehend the difference between a million and a billion pounds, because we never encounter that kind of money. I find this graphic from reddit really helpful because it demonstrates it in a simple form. £63 million sounds like a lot of money, until you compare it to the £12 billion the government have spent on an ineffective test and trace system. They seem to be able to find massive funds for public health schemes which are failing, on the one hand, whilst unable to do provide sufficient funds for programmes that we know make a very real difference, you know – feeding hungry children.
The things is that most of us find it hard to comprehend the difference between a million and a billion pounds, because we never encounter that kind of money. I find this graphic from reddit really helpful because it demonstrates it in a simple form. £63 million sounds like a lot of money, until you compare it to the £12 billion the government have spent on an ineffective test and trace system. They seem to be able to find massive funds for public health schemes which are failing, on the one hand, whilst unable to do provide sufficient funds for programmes that we know make a very real difference, you know – feeding hungry children.







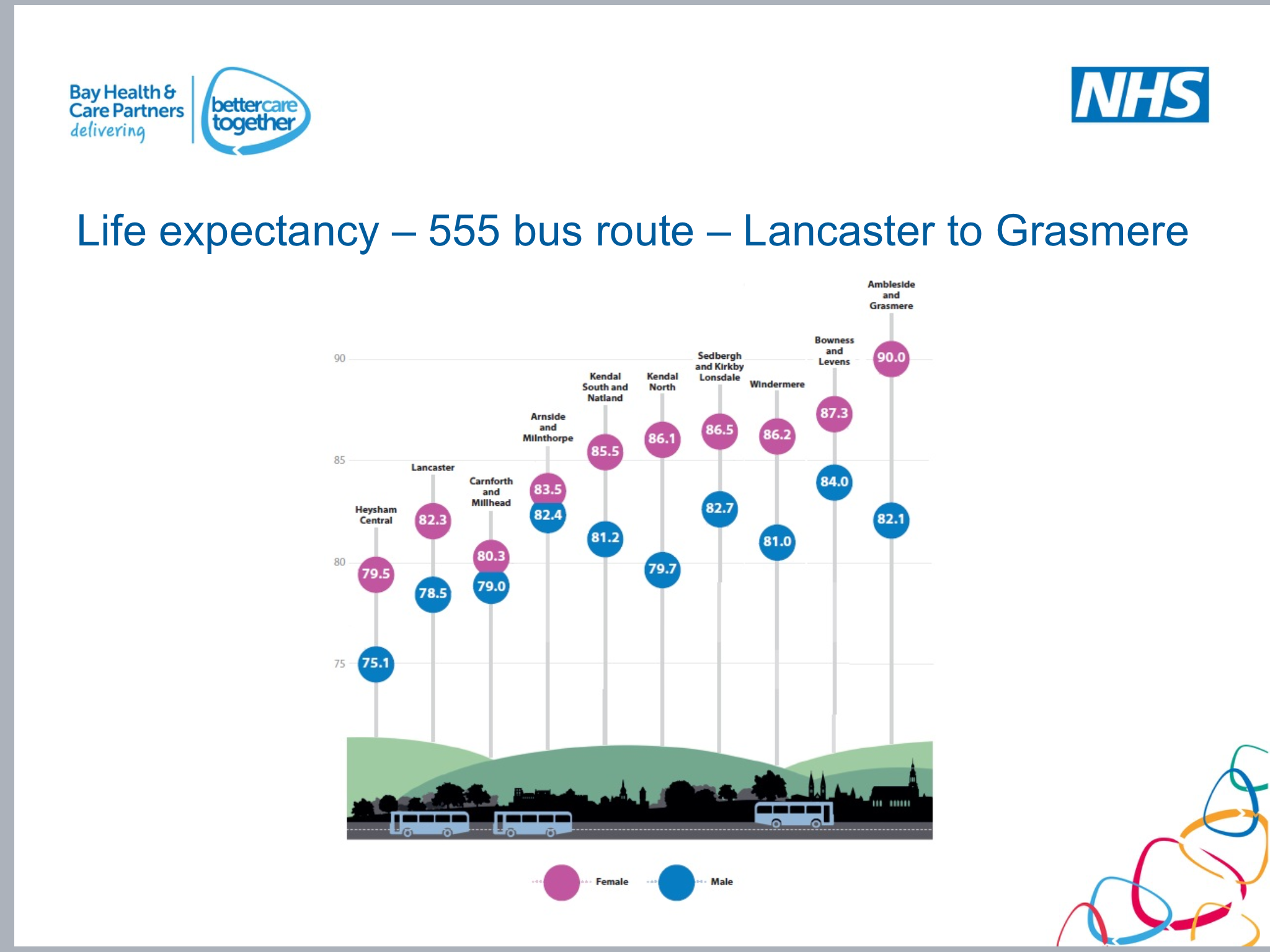



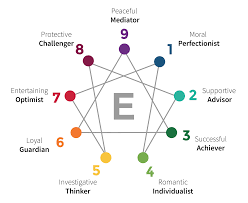

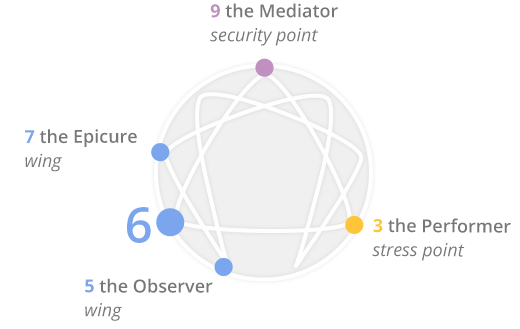
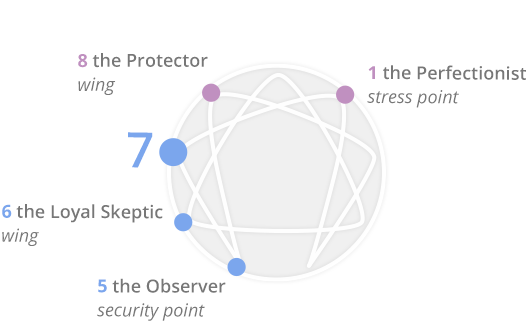

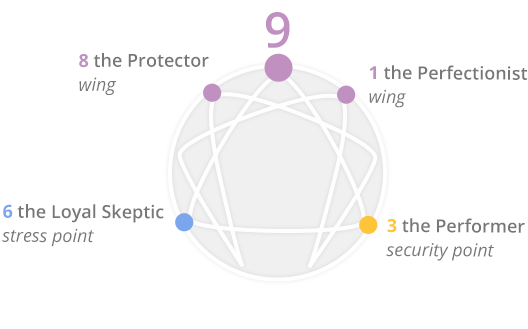






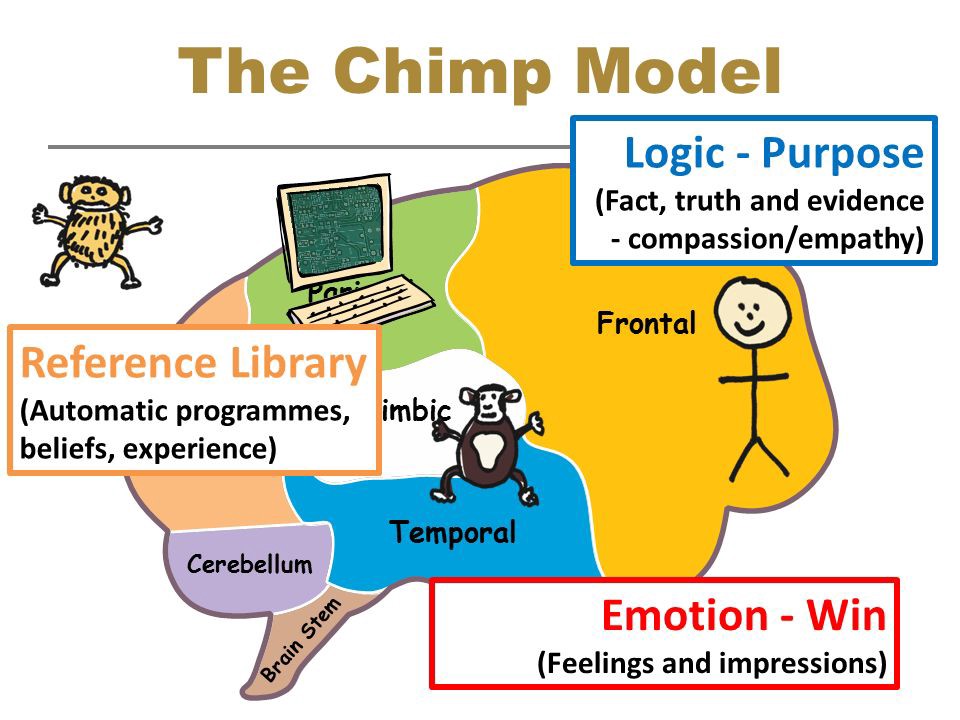




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
 – Let’s Talk About Trauma){kind=link}