Obesity has become part of a serious blame culture. “Just eat less and exercise more”, seems to be the simplistic argument these days. Social media is full of ‘fat shaming’ and the public opinion has shifted much more towards it being people’s own fault if they are fat – “they should just make better choices and take more responsibility for themselves”. It makes sense right? People just need to be a whole lot less greedy and a whole lot more restrained…..Well – just for a minute, let’s suspend our judgements, put away our pointing fingers or indeed, our shame and let’s examine the evidence….and then maybe we can have a much better and kinder conversation about the obesity epidemic we’re in and what might need to change.
A few weeks ago, I listened to the excellent Prof Sandro Galea, Knox Professor of Epidemiology at Boston State University, give an excellent lecture on: “What Do Obesity, Opioids and Guns all Have in Common?” the answer: They are all really complex and hugely important! I am shamelessly going to use his slides from that lecture to explore the issue of obesity in this blog, which Sandro has kindly shared with me.
Epidemiology at Boston State University, give an excellent lecture on: “What Do Obesity, Opioids and Guns all Have in Common?” the answer: They are all really complex and hugely important! I am shamelessly going to use his slides from that lecture to explore the issue of obesity in this blog, which Sandro has kindly shared with me.

If we take any given population, let’s start by asking this question: What percentage of obesity is determined by genetics, compared to the environment? Go, on, give it a go – write a figure down, or make a mental note of what you currently presume!
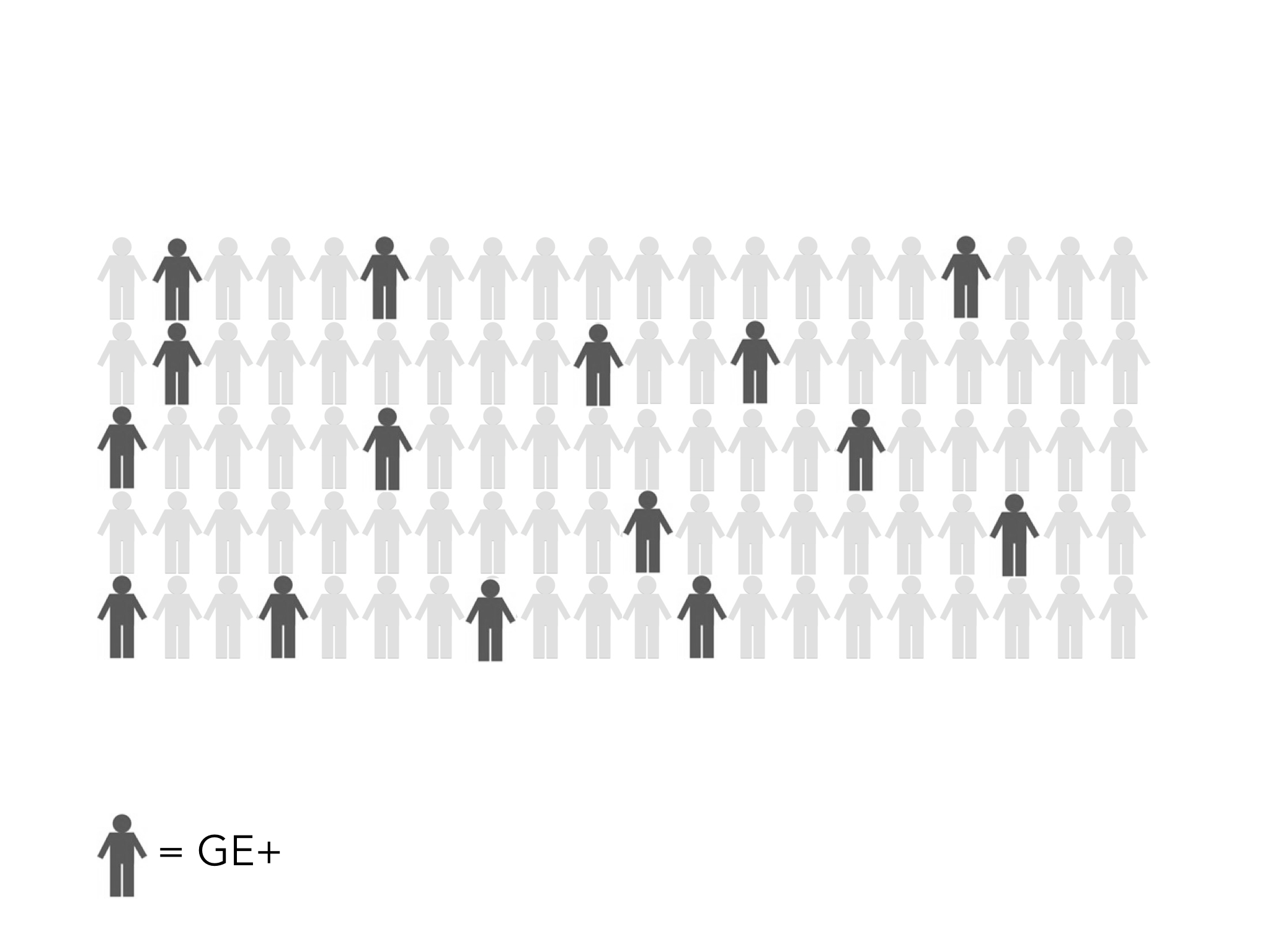
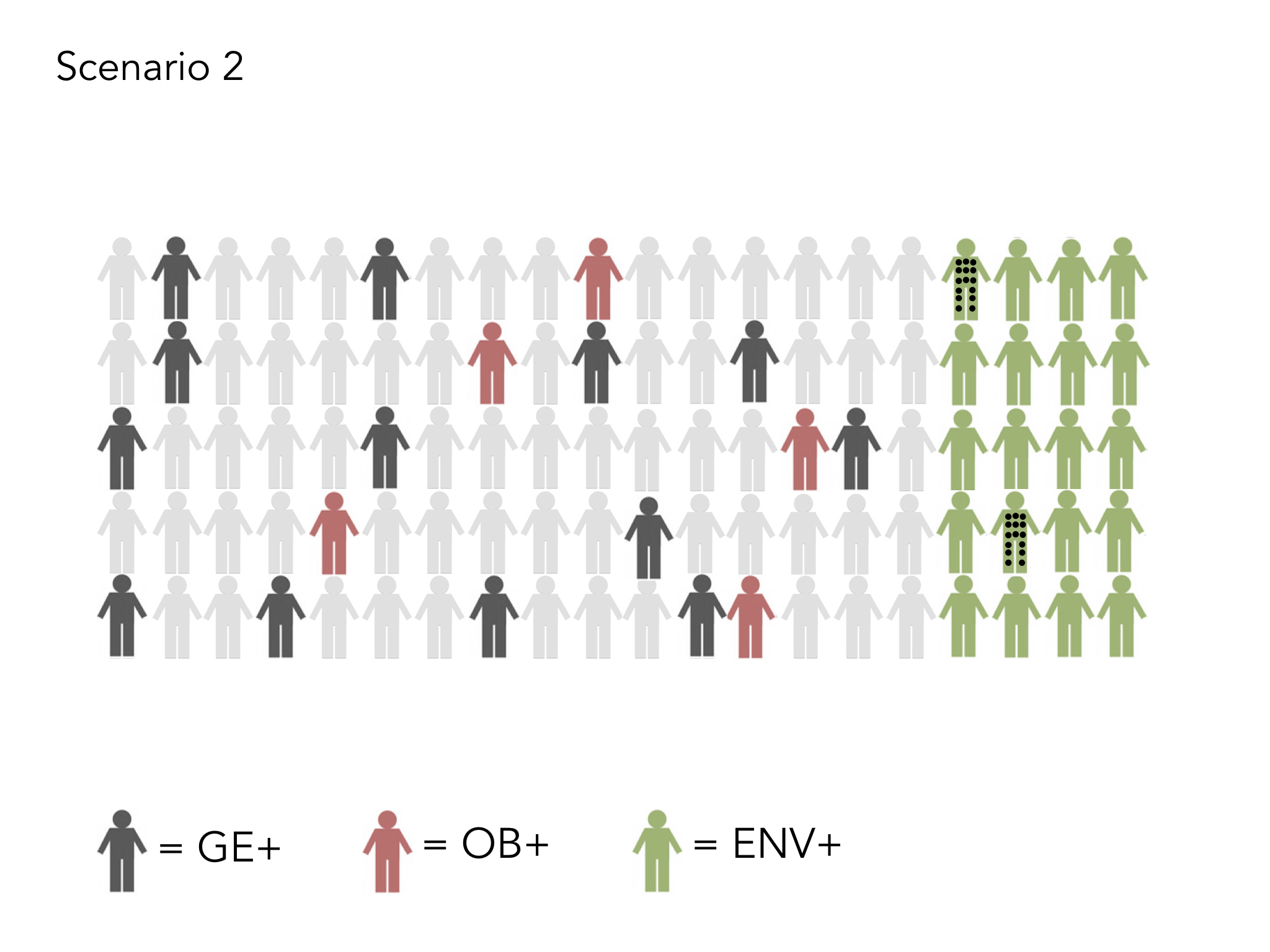
In any give population, there will be a percentage of people who have a higher genetic risk of becoming obese. In the diagrams which follow, these, dark grey represents those with a high genetic risk.
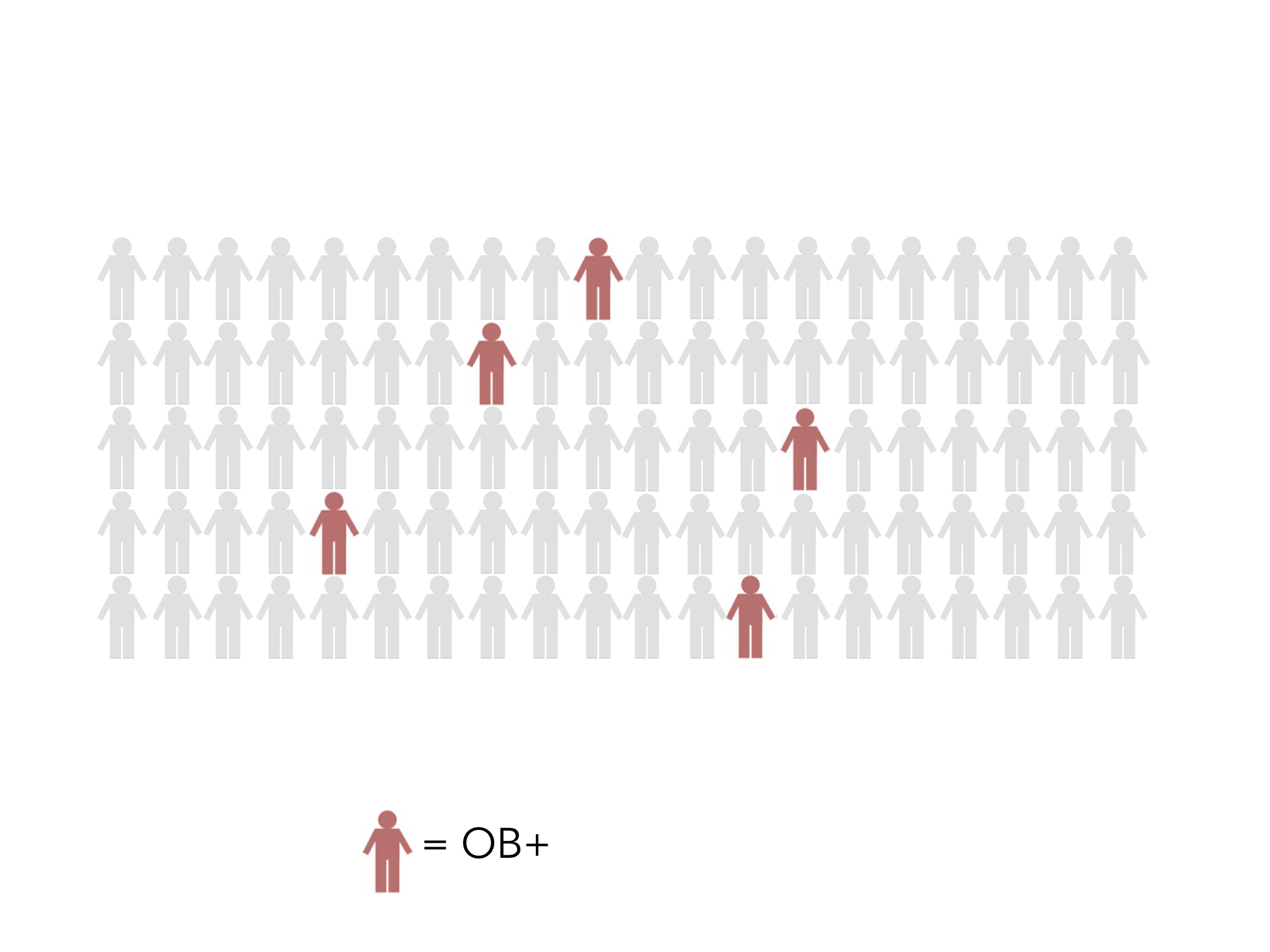
There will be some people who will be obese, with or without a genetic risk. In the following diagrams, these people are represented in red/pink.
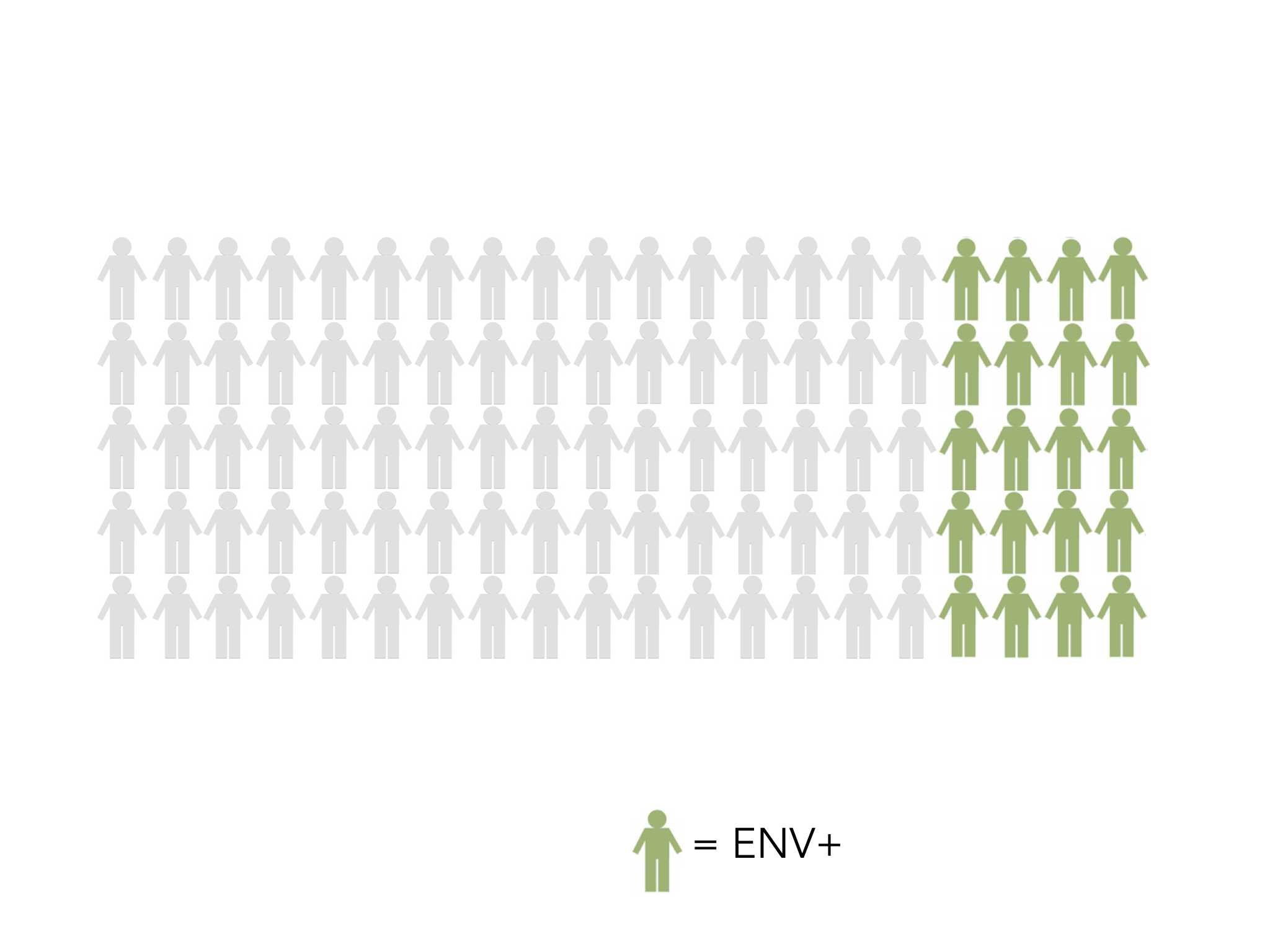
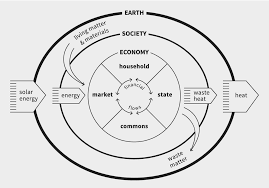
The environment is represented in green. everything that is not ‘genetic’ is considered to be environmental. This includes, air pollution, adverse childhood experiences, advertising, sugar in products, transportation, access to shops, types of shop available, family income, affordability of food, use of food banks, etc etc. The more green there is, the less healthy the environment represented.
So…….if we take a population with the same genetic risk factors and number of obese people, let’s see what happens to those people with a higher risk of becoming obese, when the environment is less than ideal, e.g. high stress, poor air quality, high index of deprivation, low educational opportunities, high unemployment, poor access to shops, poor transport links, high numbers of junk food outlets…….etc – here is the population in a poor environment and those with a genetic risk factor are marked with grey dots:
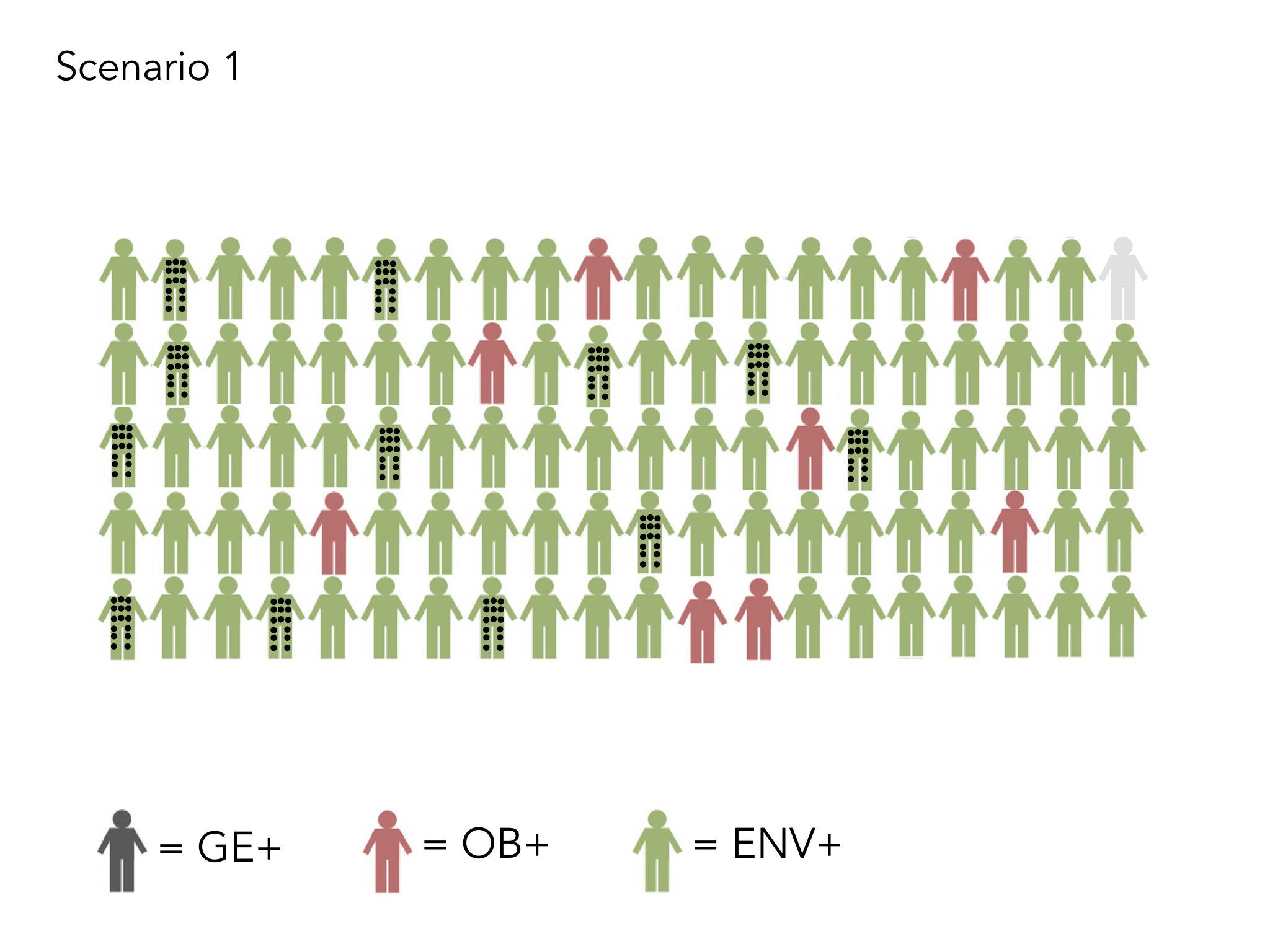
Look at what happens to the obesity rate in that population!! All of those with a genetic risk factor become obese! The odds are stacked against them, because their choices are significantly reduced!

But take the scenario, with the same population in an environment which is much more positive, where there is less sugar in foods, where there are more healthy opportunities for good eating and exercise, where there is no need for food banks because employment is high, jobs are well paid and the welfare state is functioning appropriately.
In this scenario – the odds are in favour of those genetically more likely to become obese – BIGTIME! Obesity rates are far less and overall the population is much more physically healthy. People who are genetically at risk of becoming obese have far less chance of actually becoming obese!
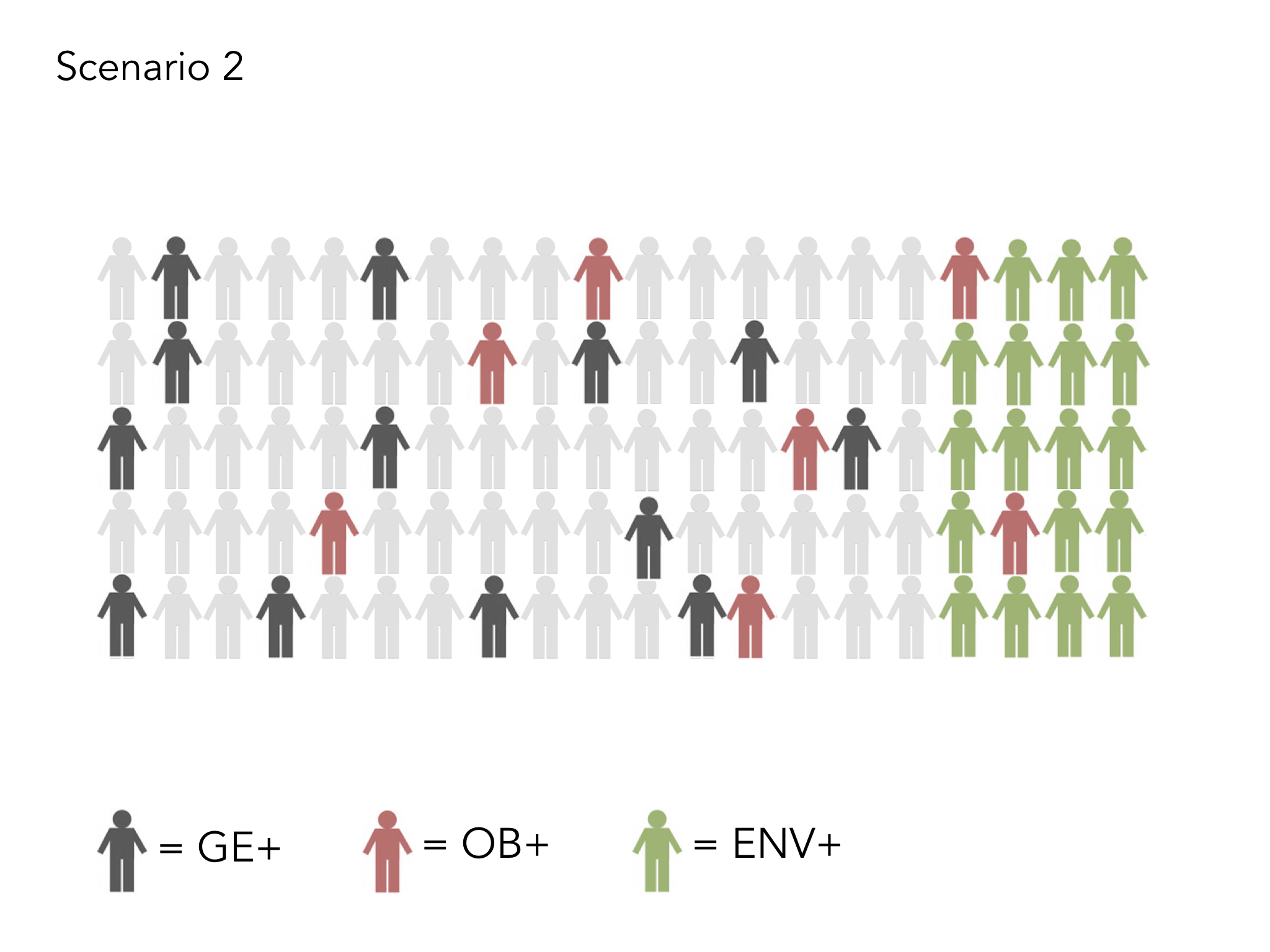
What was your answer to the percentage question at the start? It was a trick question! the worse your environment is, the more your genetics come into play! So, now there’s a complex argument about who is responsible for the environments in which we live and who creates an atmosphere of choice!
 If we take the food industry to start with, just look at what has happened to the calorie intake of foods sold in fast food outlets over the last 20 years. If you want French Fries now, you’re eating triple the calories that you were 20 years ago, due to larger portion sizes – always upsold in McDonalds (and other like minded companies)!! TRIPLE the calories! Who’s fault is that?! A turkey sandwich, which some might consider a ‘healthy option’ is now packed with more than DOUBLE the calories that were in that same sandwich just 20 years ago! Do the maths! The way this has been allowed to happen is appalling. The government, so keen on not being a ‘nanny state’ have allowed a deregulated ‘nanny food industry’ to lovingly shove calories down our throats without most of us even realising! Prof Susan Jebb, one of the leading experts in this field, globally is really clear – if we taxed cakes and biscuits and made healthy food more affordable, we would be in half the mess we’re in.
If we take the food industry to start with, just look at what has happened to the calorie intake of foods sold in fast food outlets over the last 20 years. If you want French Fries now, you’re eating triple the calories that you were 20 years ago, due to larger portion sizes – always upsold in McDonalds (and other like minded companies)!! TRIPLE the calories! Who’s fault is that?! A turkey sandwich, which some might consider a ‘healthy option’ is now packed with more than DOUBLE the calories that were in that same sandwich just 20 years ago! Do the maths! The way this has been allowed to happen is appalling. The government, so keen on not being a ‘nanny state’ have allowed a deregulated ‘nanny food industry’ to lovingly shove calories down our throats without most of us even realising! Prof Susan Jebb, one of the leading experts in this field, globally is really clear – if we taxed cakes and biscuits and made healthy food more affordable, we would be in half the mess we’re in.

The same is true of exercise, and so opportunities to exercise, created by culture and environment are really important:
If you look at how much the advertising industry is spending on obesogenic foods, or you examine where junk food cafes are placed (disproportionately higher in our most deprived communities); if you consider the profound effect of adverse childhood experiences on our eating habits or look at the affordability of health food for low income families, as shown by the food foundation, then you begin to see that this over simplistic argument that people ‘should just take more responsibility for their own health’ is total nonsense. We need to take an altogether more kind and considered view to what is an incredibly complex situation.
Sandro Galea talks powerfully about this principle: Small changes in ubiquitous causes may result in more substantial change in the health of populations than larger changes in rarer causes.
You can feed your goldfish the best food, ensure they swim their mile a day, help them practice mindfulness every morning and decrease the amount of time they spend on screens……but if you don’t care for the quality of the water – they will die!
Health inequality between the rich and poor in the UK is worsening. Health inequality between the north and south is worsening. Life expectancy overall and healthy life expectancy are both beginning to fall. Our mental health crisis is deepening. Now is not the time for loads more programmes that benefit the already healthy and make the inequalities even worse. Now is the time to ask some fundamentally deeper and more difficult questions about what we have built our society on, what the point of the government is and how, together, we might work for a future that is better for everyone. Unless we do so, the NHS continues to stare into an abyss, as indeed do all our public services.











 In my last blog, I talked about the exponential potential of what could be possible if clinicians worked together in a more collaborative way. However, far more can be achieved if we work together in and with our communities to create a social movement together around being more healthy and well. I’ve talked previously about the “battle royale” that occurred between Béchamp and Pasteur over whether we should promote health or fight disease. The answer is, of course, that we need to do both, but the clinical community is not equipped with the resource or power to do it alone.
In my last blog, I talked about the exponential potential of what could be possible if clinicians worked together in a more collaborative way. However, far more can be achieved if we work together in and with our communities to create a social movement together around being more healthy and well. I’ve talked previously about the “battle royale” that occurred between Béchamp and Pasteur over whether we should promote health or fight disease. The answer is, of course, that we need to do both, but the clinical community is not equipped with the resource or power to do it alone. crises we now face are too much for us to do anything about. We are in the midst of a battle, which we are currently losing and it is time to gird our loins for a turning of the tide. Here in Morecambe Bay, we have started a conversation, not just among the Clinical Community but with the wider population about how we might become the healthiest place in the UK. Yes, we mean this in a very holistic way, but there are also some specific foci we have so we can together reverse some of the appalling health statistics we are facing.
crises we now face are too much for us to do anything about. We are in the midst of a battle, which we are currently losing and it is time to gird our loins for a turning of the tide. Here in Morecambe Bay, we have started a conversation, not just among the Clinical Community but with the wider population about how we might become the healthiest place in the UK. Yes, we mean this in a very holistic way, but there are also some specific foci we have so we can together reverse some of the appalling health statistics we are facing. I suggest that within a generation, if we wanted to, we could render Type 2 Diabetes a rare diagnosis. We can do this through encouraging far more healthy lifestyles in our children and young people now, like running a mile a day and learning to eat food that doesn’t actually harm them! I believe we could significantly reduce the need for so many people to be taking medication for hypertension and diabetes now, prevent many strokes and heart attacks, by being violent towards these conditions with major changes in lifestyle, though diet and exercise, rather than the prescription of drugs, using coaching, peer support and local champions to give psychological motivation and encouragement. We are beginning to have some excellent discussions and develop some exciting plans around this.
I suggest that within a generation, if we wanted to, we could render Type 2 Diabetes a rare diagnosis. We can do this through encouraging far more healthy lifestyles in our children and young people now, like running a mile a day and learning to eat food that doesn’t actually harm them! I believe we could significantly reduce the need for so many people to be taking medication for hypertension and diabetes now, prevent many strokes and heart attacks, by being violent towards these conditions with major changes in lifestyle, though diet and exercise, rather than the prescription of drugs, using coaching, peer support and local champions to give psychological motivation and encouragement. We are beginning to have some excellent discussions and develop some exciting plans around this. pull themselves back from the brink of a lifetime of medication and we should use all medication reviews as a chance to help people adopt lifestyles that might reverse the need for such drugs. In the process, we would also significantly reverse our number of cancer diagnoses – many of which are linked to our lifestyle choices. We simply can’t afford for our current and failing approach to continue. We need to be braver together! And this means the NHS must be willing to partner in new ways, not only with local people, but also with businesses like the major supermarkets to help reverse our current direction towards the abyss, in which there is no longer a healthcare system that serves the needs of everyone, no matter where they come from or how much they do or don’t earn.
pull themselves back from the brink of a lifetime of medication and we should use all medication reviews as a chance to help people adopt lifestyles that might reverse the need for such drugs. In the process, we would also significantly reverse our number of cancer diagnoses – many of which are linked to our lifestyle choices. We simply can’t afford for our current and failing approach to continue. We need to be braver together! And this means the NHS must be willing to partner in new ways, not only with local people, but also with businesses like the major supermarkets to help reverse our current direction towards the abyss, in which there is no longer a healthcare system that serves the needs of everyone, no matter where they come from or how much they do or don’t earn. We can absolutely do this!! It’s going to take some serious resolve and we’re going to have to withstand the fear and pressure of some pretty powerful lobbies, like the sugar, alcohol, tobacco and pharmaceutical giants, and perhaps even the government itself, but it is time for us to do the impossible. With love, hope and faith, we can do this! Yes we need to focus on schools and work places. Yes, we need to partner with organisations we’ve never worked with before. Yes, we need a far more effective media strategy and yes, we need to allow clinicians to work very differently. But we cannot do nothing. So let’s try something a whole lot more radical. That’s what we’re going for in Morecambe Bay – not just better care together, but better health together – you can watch and wait, and see if we sink or swim, or you can join us!
We can absolutely do this!! It’s going to take some serious resolve and we’re going to have to withstand the fear and pressure of some pretty powerful lobbies, like the sugar, alcohol, tobacco and pharmaceutical giants, and perhaps even the government itself, but it is time for us to do the impossible. With love, hope and faith, we can do this! Yes we need to focus on schools and work places. Yes, we need to partner with organisations we’ve never worked with before. Yes, we need a far more effective media strategy and yes, we need to allow clinicians to work very differently. But we cannot do nothing. So let’s try something a whole lot more radical. That’s what we’re going for in Morecambe Bay – not just better care together, but better health together – you can watch and wait, and see if we sink or swim, or you can join us! It’s all over our news today – our health is in a real mess, and this is our wake-up call moment – we really do need to take it seriously. It’s all very well us protesting about the under-funding and under-recruitment in our NHS (and we are right to do so), but we can no longer shy away from the burden our own health choices are planting on the NHS. I’m telling you, it’s a mess and we have to do something, because genuinely, if we don’t there won’t be an NHS left for our children or their children. We simply cannot afford for 80% of us aged 40-60 to be overweight, exercising too little or drinking too much alcohol. We cannot afford to be spending 1 in every 5 pounds in the NHS as a direct result of our lifestyles or 1 in every 11 pounds on diabetes.
It’s all over our news today – our health is in a real mess, and this is our wake-up call moment – we really do need to take it seriously. It’s all very well us protesting about the under-funding and under-recruitment in our NHS (and we are right to do so), but we can no longer shy away from the burden our own health choices are planting on the NHS. I’m telling you, it’s a mess and we have to do something, because genuinely, if we don’t there won’t be an NHS left for our children or their children. We simply cannot afford for 80% of us aged 40-60 to be overweight, exercising too little or drinking too much alcohol. We cannot afford to be spending 1 in every 5 pounds in the NHS as a direct result of our lifestyles or 1 in every 11 pounds on diabetes. Do you know who doesn’t care? The sugar giants – they don’t care – they are more than happy to keep our kids eating a bath-full of sugar every year, and they are more than happy to take the lovely tax breaks from our government and not even contribute to the cost our NHS picks up on their behalf. The Chocolate industry – they too are pretty happy that chocolate is no longer a luxury (people used to have it as a real treat) and that we are so willing to turn a blind eye to the fact that their empires are built on the slavery of children, whilst we fulfill our insatiable greed. Who else doesn’t care? The Alcohol industry – they do not care that every time you drink one pint of beer, you are eating the equivalent of 16 fingers of kit-kat in one go – so a night out with 4 pints is 64
Do you know who doesn’t care? The sugar giants – they don’t care – they are more than happy to keep our kids eating a bath-full of sugar every year, and they are more than happy to take the lovely tax breaks from our government and not even contribute to the cost our NHS picks up on their behalf. The Chocolate industry – they too are pretty happy that chocolate is no longer a luxury (people used to have it as a real treat) and that we are so willing to turn a blind eye to the fact that their empires are built on the slavery of children, whilst we fulfill our insatiable greed. Who else doesn’t care? The Alcohol industry – they do not care that every time you drink one pint of beer, you are eating the equivalent of 16 fingers of kit-kat in one go – so a night out with 4 pints is 64 fingers of kit-kat in one evening – think about it! And by the way, they don’t pay their fair share of tax either, and yet what they cost our country is far more than they contribute. ….Then let’s not even go there with the huge Pharmaceutical giants, who are rubbing their hands together at the thought of how many of us will be prescribed medication for blood pressure, cholesterol and diabetes over the next couple of decades, when we could all do without most of it, if we made some simple changes now! And what of the Fast Food outlets that cram our high streets with ill-health choices – who makes these decisions about town planning?!
fingers of kit-kat in one evening – think about it! And by the way, they don’t pay their fair share of tax either, and yet what they cost our country is far more than they contribute. ….Then let’s not even go there with the huge Pharmaceutical giants, who are rubbing their hands together at the thought of how many of us will be prescribed medication for blood pressure, cholesterol and diabetes over the next couple of decades, when we could all do without most of it, if we made some simple changes now! And what of the Fast Food outlets that cram our high streets with ill-health choices – who makes these decisions about town planning?!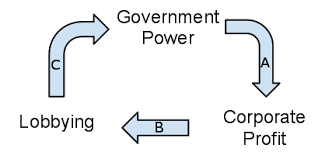 So, if these corporate giants don’t care, we should care – and maybe we haven’t until now, but it’s time we did!! And we should be pretty angry about the fact that successive governments have been on the side of greedy corporations, who are literally poisoning us. They have chosen, time and again, to support big business and the unaccountable growth of their money, above the wellbeing of their own people! And these companies have advertised the benefits of their delicacies, placed their products very carefully in collusion with the Supermarket giants and who are the fools who believed it all? That would be us! But we must not let our anger be a cause to blame someone else. We must fess up to our own weaknesses and vices, understand them and no longer let them rule us. We have been led right down the garden path of temptation, succumb to the the idea that we’re worth it and we can have whatever we want, without thinking of the consequences…..well…..now we’re at the tipping point. So let’s wake up!
So, if these corporate giants don’t care, we should care – and maybe we haven’t until now, but it’s time we did!! And we should be pretty angry about the fact that successive governments have been on the side of greedy corporations, who are literally poisoning us. They have chosen, time and again, to support big business and the unaccountable growth of their money, above the wellbeing of their own people! And these companies have advertised the benefits of their delicacies, placed their products very carefully in collusion with the Supermarket giants and who are the fools who believed it all? That would be us! But we must not let our anger be a cause to blame someone else. We must fess up to our own weaknesses and vices, understand them and no longer let them rule us. We have been led right down the garden path of temptation, succumb to the the idea that we’re worth it and we can have whatever we want, without thinking of the consequences…..well…..now we’re at the tipping point. So let’s wake up! This situation exposes something far deeper than just an argument between Jeremy Hunt and the BMA and is far more important than discovering who has the strongest will power. Infact, the BMA have made a major error in targeting Jeremy Hunt so vindictively, because in the final analysis, this isn’t about Hunt at all. Jeremy Hunt can be replaced in a moment, and is likely to be succeeded by a far more robust
This situation exposes something far deeper than just an argument between Jeremy Hunt and the BMA and is far more important than discovering who has the strongest will power. Infact, the BMA have made a major error in targeting Jeremy Hunt so vindictively, because in the final analysis, this isn’t about Hunt at all. Jeremy Hunt can be replaced in a moment, and is likely to be succeeded by a far more robust  Boris Johnson, who will simply pound his fist more visciously. To make Hunt the scape goat narrows this debate to something far too insignificant and actually strengthens the government’s ability to do exactly as they please.
Boris Johnson, who will simply pound his fist more visciously. To make Hunt the scape goat narrows this debate to something far too insignificant and actually strengthens the government’s ability to do exactly as they please. place, the goverment could instead have said to all the hospital trusts across the country what their hopes and intentions were and then waited to see if this was workable, in what way and how much it would cost. But you cannot simply act like Pharoah and expect the brick makers to make ever more bricks with less and less resource available – otherwise, you face an exodus!
place, the goverment could instead have said to all the hospital trusts across the country what their hopes and intentions were and then waited to see if this was workable, in what way and how much it would cost. But you cannot simply act like Pharoah and expect the brick makers to make ever more bricks with less and less resource available – otherwise, you face an exodus! The system, to which we must all bow doesn’t care for the needs of the people who work within it. It will force them to submit. Why should doctors (many of whom work for less than the minimum wage, when on call) be allowed time to rest at weekends? Why can’t everybody have routine care through the weekend, just as from monday to friday (even though most of our top clinicians think we need better emergency care and not routine access)? Surely our economy needs this kind of health service? And actually, whilst we’re on it, isn’t it a waste of time, allowing teachers to have weekends off as well? Don’t we need our children to work harder, or at least be given some sort of babysitting service, so we can get more for our pound of flesh from their parents? If we are to have a 24/7 health service, why not a 24/7 education service? Our shops are already open practically 24/7. In this commercial world – shouldn’t everything else follow suit? No, no and NO!!
The system, to which we must all bow doesn’t care for the needs of the people who work within it. It will force them to submit. Why should doctors (many of whom work for less than the minimum wage, when on call) be allowed time to rest at weekends? Why can’t everybody have routine care through the weekend, just as from monday to friday (even though most of our top clinicians think we need better emergency care and not routine access)? Surely our economy needs this kind of health service? And actually, whilst we’re on it, isn’t it a waste of time, allowing teachers to have weekends off as well? Don’t we need our children to work harder, or at least be given some sort of babysitting service, so we can get more for our pound of flesh from their parents? If we are to have a 24/7 health service, why not a 24/7 education service? Our shops are already open practically 24/7. In this commercial world – shouldn’t everything else follow suit? No, no and NO!! This is why we need a revolution of solidarity and resistance. We need a people movement who will stand together and be brave enough to say that there is a different way to see the world and a new way to live within it. Our naked life itself, although currently abused, can become for us our greatest power. Our naked life can expose the truth of just how abusive our systems have become. Our naked life, when combined with the indestructable force of kenotic love, becomes the very agent of change that we need.
This is why we need a revolution of solidarity and resistance. We need a people movement who will stand together and be brave enough to say that there is a different way to see the world and a new way to live within it. Our naked life itself, although currently abused, can become for us our greatest power. Our naked life can expose the truth of just how abusive our systems have become. Our naked life, when combined with the indestructable force of kenotic love, becomes the very agent of change that we need. really demonstrate the power of naked life……how about naked marches?!! (I grew up in Coventry, and so the story of Lady Godiva is in my blood – nakedness overcame oppression once before!). Or maybe the staff of the NHS should all turn up to work with no clothes on?!! How about people stripping off at least to their underwear to expose both the fragility and the power of naked life?!
really demonstrate the power of naked life……how about naked marches?!! (I grew up in Coventry, and so the story of Lady Godiva is in my blood – nakedness overcame oppression once before!). Or maybe the staff of the NHS should all turn up to work with no clothes on?!! How about people stripping off at least to their underwear to expose both the fragility and the power of naked life?!{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}