Last week I had the complete joy (except for the awfulness that is the M6 and M62!) of heading over to Hull to speak at a gathering of Public Health and Public Sector people from across Yorkshire, The Humber and The East Riding, called “Minding the Gap”, hosted by the amazing Ian Copley. In my next blog, I will give the podcast of what I said and written piece, for those who prefer that format, about Population Health and the realities we are currently facing.
However, I thought it just worth reflecting on a really interesting lecture I heard by Prof Franco Bianchini from Hull University (https://www.hull.ac.uk/work-with-us/research/institutes/culture-place-and-policy-institute/culture-place-and-policy-institute.aspx) on the impact of Hull being European City of Culture 2017. It was amazing to see this little video, presented by the excellent Director of Public Health, Julia Weldon (https://www.yhphnetwork.co.uk/about-us/julia-weldon/), and to hear of so many wonderful, creative, life-giving, community-building initiatives that happened all over the City and the beautiful stories of people celebrating the history and many facets of this place.
The sense of wellbeing and happiness in the City increased significantly during that year (not much of a surprise) and the injection of finance into Hull gave opportunity for some creative regeneration and fantastic projects. Unfortunately, since 2017, the overall sense of Wellbeing and happiness has now fallen to below what it was in the years preceding Hull as the City of Culture. What a shame! And interestingly, if you study other Cities that host Olympics, Commonwealth Games, or have other similar initiatives, you see the same pattern over and over. The hype wanes, the carnival moves on and what is left?
There is so much we can learn from this, if we want to. Firstly, if we only plan for an event and do not think about it as an agent of transformation for the future, then we risk sowing huge promise and then once the event finishes, things just go back to being the same old, breeding disappointment and disillusionment. This must be taken into account in the planning. Becoming a City of Culture gives the opportunity for a City to come together, not only for an event, but to turn the future of the city, releasing dreams of what it can become. This requires much wider ownership and community conversations about keeping the momentum and building on it. Secondly, leaders across the city need to own the future and hold true to the principles, especially once the funding is withdrawn. It’s really sad that the vast majority of schools have not felt able to continue the great initiatives in the creative arts or sports, which began and were having a great effect on children and young people’s physical and mental health, due to the pressures they feel around delivery of the curriculum. Surely there was an opportunity to reimagine the whole realm of what education might look like in the City of Hull, aligned to the values of the City and its hope for the future?
In the Jewish tradition, at certain points along their journey from Egypt to Israel, the people would build an ‘Ebenezer’. It was a pile of stones to mark a certain point on their journey that would help them remember what was past and what they were looking forward to. It was more than a monument. It was a stake in the ground which called to memory where they had come from, what they had been through but also opened up an altogether different future. My hope for Hull, is that 2017 City of Culture becomes an Ebenezer for the city, something they can look back on and say – “that’s when things really began to change, that’s when we celebrated our past but began to build a new future together, a city that really works for everyone and the environment we live in!” I fear, however, that the opposite will be true….a temporary flash in the pan and then back to the same old, same old……
I hope with all my heart that it isn’t too late for Hull to regain this momentum and despite the lack of funding (although this begs whole new questions about devolution) for the city to take hold of the promise of what could be. I also really hope that Coventry (the city of my birth) really hears and learns from the lessons of Hull and begins now to think of being the City of Culture 2021 to springboard into a new future for the city, rather than have yet another event that feels good in the moment, but does not bring the transformation of the City that is so desperately needed. Now is the time for Coventry to dream and to think creatively about what this opportunity really might become.
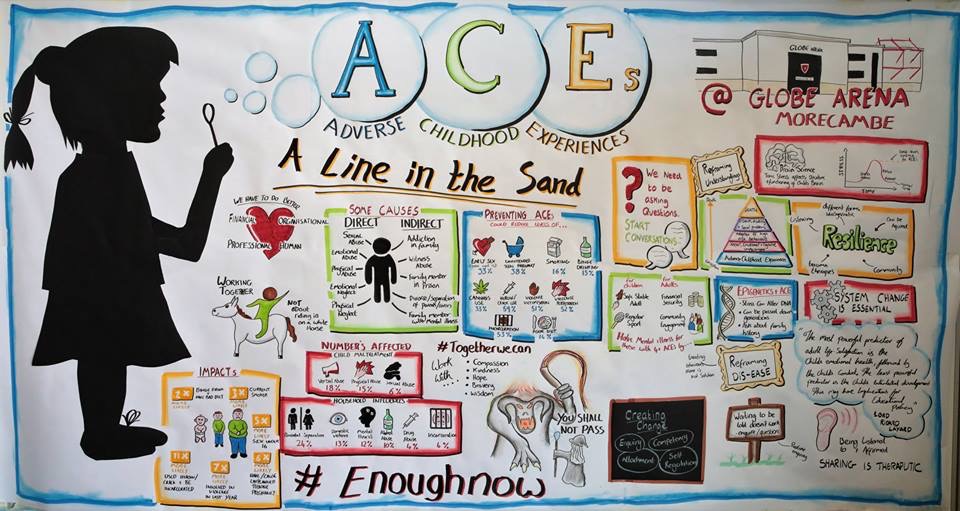
Last week, I had the utter privilege of co-hosting a conference with my good friend, Siobhan Collingwood, the head teacher at Morecambe Bay Community Primary School on Adverse Childhood Experiences (ACEs), at the Globe Arena. We both know the reality of ACEs every day in our communities (see my previous blog) and so wanted to bring people together from across our amazing community in North Lancashire, working in the public and community sector, or simply with a passion to see change, to explore how we can begin to say “Enough Now” to ACEs. (Huge thanks to the incredible Jon Dorsett for his graphic art).
As part of the day, my friends, Ian Cooper (Chief Inspector of Police) and Nick Howard (who leads the team at the city council on housing and planning) hosted a 135 minute conversation for all 180 participants around this theme: ‘Together, what can we do to transform the experience of childhood for good?’ There was such a buzz as people from different backgrounds and perspectives, collaborated and challenged each other to break out of our boxes and find new ways to bring transformation. The ideas generated were incredible and each person left the room with a clear commitment and next step for what they needed to do in their place of work or neighbourhood. Already we are hearing amazing stories and initiatives which are beginning as a result and we are building networks together.
We had fantastic input from Prof Warren Larkin, Sue Irwin (and her excellent work with EmBRACE), and host of other brilliant people working across many sectors, lending their expertise to further the conversations in interactive seminars – the feedback on each one has been incredible!
So – there is a huge challenge to the English Government (Scotland, Wales and Northern Ireland are already streaks ahead) as to why they are not taking the vast evidence base seriously and playing their part in breaking this devastating cycle. If we are to tackle this enormous issue of ACEs, it means vast changes to the ways we are delivering and measuring education in our schools and a serious reassessment of cuts of funding to children’s centres, midwives and health visitors, removing target-driven outcomes and finding ways to put relationship back into the heart of our modus operandi. It will take a people movement to bring the shifts that are needed, but given just how devastating ACEs are to physical, mental, emotional and social wellbeing and the huge cost burden they are to our public services and society, we have to give ourselves to drawing a line in the sand, saying enough now and reimagining the future together.
Here in Morecambe Bay, and across Lancashire, we are taking this issue really seriously and believe it to be one of THE most important population health issues of our time. A few of us have co-authored a ‘Little Book of ACEs’ together, in conjunction with Lancaster University – available very soon (!) which you might find helpful. My section expands a little on a previous blog post I have written here.
This whole area of ACEs is so sensitive, it takes compassion, kindness, bravery and wisdom. We cannot face it alone in silos, but together we can! Together, we can bring healing to our communities and freedom for the generations to come. We have to be willing to be those, who life Gandalf, in ‘The Lord of the Rings’ take our staff and say to this Balrog, which has devoured too many lives – “you shall not pass!” We have to give ourselves to drawing a line in the sand, saying “enough now” and step into a reimagined future of childhood, together.
I recently hosted a couple of conversations for people in the city of Lancaster, UK, in which we explored this question together: “How Do We Build a City that Works for Everyone?” We framed the conversation (which we had using a ‘World Café’)from two current and important concepts. Firstly, the great work of Kate Raworth in ‘Doughnut Economics’ – how do we create a city that is socially just for the people who live here and that is environmentally sustainable for the future? In other words, how do we ensure we have an economy that is distributive and regenerative by design? Secondly, we drew on the important work of Sandro Galea (Professor of Epidemiology at Boston State) and his concept of the Goldfish bowl as a way of thinking about ‘Population Health’ or Epidemiology (see my last blog). Politics IS health, according to Galea.
One of my favourite quotes is from Einstein, when he said that “If I had 60 minutes to save the world, I would spend 55 minutes trying to find the right question and then I could solve the problem in 5 minutes.” It turns out that the question we used itself is problematic at a few levels! Here are some of the questions we found ourselves wrestling with: Do we need to build the city, when it is already here?! What do we really mean by ‘the city’ – is it people and communities or more than that? What do we mean by ‘works for’? That felt to some like we were settling for something that was just enough, maybe scraping by, rather than thriving! And who do we mean by everyone?! This didn’t stop us having a a great discussion, but highlights how powerful the perspectives and biases we bring into the room can be!
Despite not having a perfect question, (and hopefully, by the time we host 3 much bigger conversations across the city during 2019, we may have honed something more helpful!), some key themes emerged, through our generative conversation.
Relationships are vital! We want to live in a city which really does “work” for everyone. So, we want to give value to the currently unheard voices and we want to value diversity and inclusivity. Taking time to get to know neighbours and colleagues grows a richness of community. We want to live in a city that values love and kindness in how we treat ourselves and other people.
We need to build on the amazing assets and skills that we already have in the city. If we made space and time to discover and share these skills with each other more, we would develop a richer life experience within our communities. This is an expression of ‘gift economy’ and ‘reciprocity’, which Charles Eisenstein writes powerfully about in his book ‘Sacred Economics’). It builds on voluntary power, and may require a reimagining of how we work and what we value in how we invest our time, energy and resources. We also have so many incredible physical assets in this area, which we don’t tap into enough or perhaps make fully accessible for all who live in the city.
People want to be part of the change, not have change happen to them! This requires much better engagement and democratic discussion about how budgets are spent, for example or how land is developed. Somehow, there needs to be a better safeguarding against ‘invested interests’ and ‘dodgy deals’ with far more transparency about how decisions are made. Such a process, it is believed, would enable far better personal and corporate responsibility when it comes to caring for the fabric of the city and the people who live here, similar to what has been developed in Wigan. There was a recognition that when we talk about personal choice and responsibility that this is much more possible for some people and communities than others. However, it was felt that increasing self-esteem and a sense of belonging would enable more personal responsibility and choice.
Housing really matters. The physical environment is actually causing fragmentation and silos. There were many more questions than answers here – but that’s ok – this is an iterative process, and we don’t have to solve everything in one go. So…how do we create really good social housing? How could we redesign the spaces of the city to encourage togetherness and community? How do protect green spaces in the process and take care of the city’s drainage (strong memories of the recent floods)? How could we ensure that everyone has a home to live in, and what might that mean for both the homeless and also for single people?
We want an education system that really values the unique beauty of each child, treats each one with compassion, mindful of what traumas they may be experiencing and values creativity and activity in education just as much as academic outcomes. We care about who our children become, not just about what exams they pass. So we recognise that we have a measurement problem but we’re not quite sure yet what to do about it!
We need to invest in our children and young people by providing physical spaces in which our young people can feel safe and not bored! Many have been affected by the closure of children’s and youth centres. If we are to really invest in our children and young people, there was a sense that we also need to provide parenting classes across the board to pregnant couples and through ‘family centres’ and schools across the district.
We want to create a greater sense of value for our older citizens. There were many people present who felt they have things to offer, but don’t have an obvious outlet. Involving those retired from paid work more in the life of the city would break isolation and feed the gift economy.
Business needs to thrive in a way that really values entrepreneurial gift and allows it to flourish, whilst holding it true to the ideas and principles of the doughnut and the goldfish! How could the business community serve the needs of the city and how can the city enable business to really thrive, creating jobs, whilst caring for the environment and the needs of the people who live here? Kate Raworth’s work could really help us!
Transport systems need to be redesigned to encourage more cycling and walking or the use of green public transport alternatives. Transport routes also need to join up our communities more effectively to improve opportunities for those who live in areas that are currently more financially deprived.
If we are to really improve health and wellbeing and care for the environment, then we need to see this written into EVERY policy decision. If politics IS health, as per Sandro Galea, then we need to take this seriously and stop making policies which do not care for these things.
We want to be part of city that does welfare well! We think there are many possible new ways of doing things more effectively, as described in Hilary Cottam’s book, ‘Radical Help – Reimagining the Welfare State’. One of the things felt to be important is increasing skills in money management (85% of people living in social housing in this district are in debt to the city council -though this is certainly not only due to poor money management , but an unjust system that isn’t working for the majority). Morecambe Bay Credit Union offers an alternative economy as a way of using micro finance in our local geography.
We need better ways to communicate and connect people together. There is smart, digital technology that could help us here….perhaps a Lancaster portal, that connects us together more effectively and helps facilitate the sharing of our assets and gifts.
Wowsers! Not bad for 2 conversations of 90 minutes each! Just imagine what a phenomenal city Lancaster might become over the next 10-20 years, if we set out on a journey together to build this kind of city! What is stopping us, I wonder?! #enoughnow #togetherwecan
This week, the Kingsfund, one of the most respected think-tanks on health and social care in the UK declared that the current NHS staffing levels are becoming a ‘national emergency’.
The latest figures have been published by the regulator, NHS Improvement, for the April to June period.
They showed:
■ 11.8% of nurse posts were not filled – a shortage of nearly 42,000
■ 9.3% of doctor posts were vacant – a shortage of 11,500
■ Overall, 9.2% of all posts were not filled – a shortage of nearly 108,000
This is having a profound impact on staff who are working in the NHS now, with low morale, high stress levels, increasing mental health problems and people leaving the profession (either to go over seas, where pay and work-life balance is considerably better) or retire early.
Increasing the number of doctors, nurses and midwives (all with considerable debt, mind you!), by 25% over the next 5 years is welcome, but it doesn’t solve the problem now, and it is unlikely to be enough, even then!
But, let’s take a solutions focussed approach. What can we do now? I think there are a few things we need to consider:
I can understand how frustrating it is for the public to find that waits are longer to receive much needed care. When we’re anxious or worried about our own heath or that of a loved one, we are understandably at a position of higher stress. However, this staffing crisis is not of the making of the nurses, doctors and other health professionals who work long hours every day to provide the best health care they can. So, it’s really important that as a country, we treat our NHS staff with kindness, gratitude and respect. The current abuse of NHS staff is making the job even harder and really making people not want to come to work. And that means we also need to make complaints in a way that is perhaps a bit more compassionate or understanding towards people who are working under high stress situations. It is important that we learn from mistakes, but complaints have a huge impact on staff and can hugely affect their confidence, even when they are dealt with in a very compassionate way by those in leadership.
We need to ensure that we use our appointments appropriately. Yes – sometimes, we have to wait a while to see our GP, but if we get better in the mean time, we really don’t need to be keeping the appointment! And missing appointments costs us all so much time and energy and makes those waiting lists ever longer. If we value our health system, we need to either keep appointments, or take responsibility to cancel them.
We need to take an urgent look at the working day of our NHS staff and work out how we build more health and wellbeing breaks into their days. We need staff to have space to connect, keep learning, be active, be mindful and take appropriate breaks. This means senior leadership teams getting the culture right, when the pressure is on and the stakes are high.
We need to get smarter with digital and enable patients to make better and more informed choices about their own care and treatment, with better access to their notes. In this way, we waste less time and empower people to become greater experts in the conditions with which they live everyday. There are great examples of where this is happening already. It isn’t rocket science and can be rolled out quite easily. It’s good to see some announcements about this from the new health secretary Matt Hancock MP, but we need to make sure the deals and the products are the right ones. It’s also vital, when it comes to digital solutions that Matt Hancock listens to his colleague and chair of the health select committee, Dr Sarah Wollaston MP, in being careful what he promotes and prioritises.
We need to be thinking NOW about the kind of workforce we are going to need in the next 2-3, and 5-10 years and we need to get the training and expectations right now! There is no point designing our future workforce based on our current needs. Rather, we need expert predictive analysis of the kind of future workforce we will need, in line with the ‘10 year plan’ and begin to grow that workforce now. If it’s healthcoaches we need to work alongside GP practices, then let’s get them ready, if it’s community focussed nursing teams, then let’s adjust the training programmes. This kind is vital and must influence what happens next.
We need to stop putting pressure on NHS staff to deliver that which is currently undeliverable without causing significant stress to an already overstretched workforce. By this I mean centrally driven schemes, such as the intended roll out of GPs working 8-8, 7 days a week. Maybe it’s an aspiration for the future if we can sufficiently reimagine the workforce, but it’s not a priority now and isn’t the answer to the problems we’re facing.
We need to stop the cutting of social care in local governments, and ensure that central funding flows to where it needs to be, to ensure the allied support services are present in local communities to work alongside NHS colleagues in getting the right care in the right place at the right time. This is the single biggest cause of our long ED waits and our problems with delayed discharges from hospital. It isn’t rocket science. It’s the reality of cuts to our social care provision, which have been too deep and this needs to be reversed.
Personally, although it is an option, I feel uncomfortable about a ‘recruitment drive’ from overseas, as it is very de-stabilising to health care systems in more deprived parts of the world when we do that. I think there are some win-win initiative we could develop pretty quickly that could also form part of our international development strategy.
In summary, we need to treat our NHS staff with kindness, look after their wellbeing, use our services appropriately, use digital technology with wisdom and not for political gain, redesign and start building the workforce of the future now, stop undeliverable initiatives and ensure the right funding and provision of services through social care which means central government funding back into local government. It won’t solve everything, but it will go along way towards giving us a more sustainable future to the NHS.
Applying a Population Health Approach to Adverse Childhood Experiences
Adverse Childhood Experiences are one of our most important Population Health issues due to their long lasting impact on the physical, mental and emotional health and wellbeing of a person and indeed the wider community. It is therefore really important that we apply a ‘population health’ approach in our thinking about them so that we can begin to transform the future together. This is an area of great complexity with several contributing factors and will take significant partnership across all levels of government, public bodies, organisations and communities to bring about a lasting change. There are things we can do immediately and things that will take longer, but with a growing awareness of just what a significant impact ACEs are having on our society, we must act together to do something now. Here in Morecambe Bay, we have developed a way of thinking about Population Health in what we call our ‘Pentagon Approach’. It can be applied to ACEs as a helpful framework for thinking about how we begin to turn this tide and cut out this cancer from our society and feeds into the already great work being done across Lancashire and South Cumbria, lead by Dr Arif Rajpura and Dr Helen Lowey, who have spearheaded so much!
Prevent
When we examine the list of things that pertain to ACEs (see previous https://reimagininghealth.com/facing-our-past-finding-a-better-future/ blog), it is easy to feel overwhelmed and put it into the ‘too hard to do’ box. This is no longer an option for us. We must begin to think radically at a societal level about how we prevent ACEs from happening in the first place (recognising that some ACEs are more possible to prevent than others). Prevention will entail a mixture of community grass-roots initiatives, changes in policy and a re-prioritisation of commissioning decisions for us to make a difference together. Here are some practical suggestions:
The first step is most certainly to break down the taboo of the subject and continue to raise awareness of just how common ACEs are and how utterly devastating they are for human flourishing. ACE aware training is therefore vital as part of all statutory safeguarding training.
We have to tackle health inequality and inequality in our society. ACEs, although common across the social spectrum are more common in areas of poverty. Although we now have more people in work, many people are not being paid a living wage, work settings are not necessarily healthy and child poverty has actually increased over the last 5 years in our most deprived areas https://www.jrf.org.uk/blog/poverty-taking-hold-families-what-can-we-do.
Parenting Classes should be introduced at High School in Personal and Social Education Classes to help the next generation think about what it would mean to be a good parent. These should also form an important part of antenatal and post-natal care, with further classes available in the community for each stage of a child’s development. Extra support is needed for the parents of children with special developmental or educational needs due to the increased stress levels involved.
There needs to be a particular focus on fatherhood and encouraging young men to think about what it means to father children. Recent papers have demonstrated just how important the role of a father can be (positive or negative) in a child’s life and it is not acceptable for the parenting role to fall solely to the mother. www.eani.org.uk/_resources/assets/attachment/full/0/55028.pdf
We have much to learn from the ‘recovery community’ about how to work effectively with families caught in cycles of addiction from alcohol or drugs. Finding a more positive approach to keeping families together whilst helping those caught in addictive behaviour to take responsibility for their parenting or learn more positive styles of parenting, whilst helping to build support and resilience for the children involved is really important.
We must ensure that our social services are adequately funded and that there is continuity and consistency in the people working with any given family, especially around the area of mental health. Relationships are absolutely key in bringing supportive change and we must breathe this back into our welfare state.
Hilary Cottam writes powerfully in her book, Radical Help that we must foster the capabilities of local communities, making local connections and “above all, relationships”. As Cottam states, “The welfare state is incapable of ‘fixing’ this, but it has an important role to play. It can catch us when we fall, but it cannot give us flight.
Sex education in schools needs to be more open and honest about the realities of paedophilia and developing sexual desire. Elizabeth Letourneau argues powerfully that paedophilia is preventable not inevitable. We must break open this taboo and start talking to our teenagers about it. (https://www.tedmed.com/talks/show?id=620399&utm_source=rss&utm_medium=rss)
Detect
If we want to make a real difference to ACEs and their impact on society, we need to be willing to talk about them. We can’t detect something we’re not looking for. Therefore as our awareness levels rise of the pandemic reality of ACEs, we need to develop ways of asking questions that will enable children or people to ‘tell their story’ and uncover things which may be happening to them or may have happened to them which may be deeply painful, or of which they may have memories which are difficult to access. Again, our approach needs to be multi-level across many areas of expertise. We need to be willing to think the unthinkable and create environments in which children can talk about their reality. For children in particular, this may need to involve the use of play or art therapy.
Whole school culture change is vital, with a high level of prioritisation from the school leadership team is needed to ensure this becomes everybody’s business.
School teachers and teaching assistants need to be given specific training, as part of their ‘safeguarding’ development about how to recognise when a child may be experiencing an ACE and how to enable them to talk about it in a non-coercive, non-judgmental way.
Police and social services need training in recognising the signs of ACEs in any home they go into. For example, in the case of a drug-related death, how much consideration is currently given to the children of the family involved, and how much information is shared with the child’s school so that a proactive, pastoral approach can be taken. There are good examples around England where this is now beginning to happen. (http://www.eelga.gov.uk/documents/conferences/2017/20%20march%202017%20safer%20communities/barbara_paterson_ppt.pdf)
For adults, we need to recognise where ACEs might have played a part in a person’s physical or mental health condition (remember the stark statistics in the previous blog on this subject). Therefore we need to develop tools and techniques to help people open up about their story and perhaps for clinicians to learn how to take a ‘trauma history’.
Clinical staff working in healthcare need to be given REACh training (routine enquiry about adverse childhood experiences – Prof Warren Larkin) as part of their ongoing Continuous Professional Development (CPD). In busy clinics it is easier to focus on the symptoms a person has, rather than do a deeper dive into what might be the cause of the symptoms being experienced. A wise man once said to me, “You have to deal with the root and not the fruit”. Learning to ask open questions like “tell me a bit about what has happened to you” rather than “what is wrong with you”, can open up the opportunity for people to share difficult things about their childhood, which may be profoundly affecting their physical or mental health well into adulthood. There is a concern that opening up such a conversation might lead to much more work on the part of the clinician, but studies have shown that simply by giving someone space to talk about ACEs they have experienced, they will subsequently reduce their use of GPs by over 30% and their use of the ED by 11%.
We can ask each other. This issue is too far reaching to be left to professionals. If simply by talking about our past experiences, we can realise that we are not alone, we are not freaks and we do not have to become ‘abusers’ ourselves, then we can learn to help to heal one another in society. Caring enough to have a cup of tea with a friend and really learn about each other’s life story can be an utterly healing and transformational experience. When we are listened to by someone with kind and fascinated, compassionate eye, we can find incredible healing and restoration. One very helpful process, ned by the ‘more to life’ team is about processing life-shocks. Sophie Sabbage has written a really helpful book on this, called ‘Lifeshocks’).
Protect
When a child is caught in a situation in which they are experiencing one or more ACE, we must be vigilant and act on their behalf to intervene and bring them and their family help. When an adult has disclosed that they have been through one or more ACE as a child, we must enable them to be able to process this and not let them feel any sense of shame or judgement.
We need to ensure school teachers are more naturally prone to thinking that ‘naughty’ or ‘difficult’ children are actually highly likely to be in a state of hyper vigilance due to stressful things they are experiencing at home. Expecting them to ‘focus, behave and get on with it’, is not only unrealistic, it’s actually unkind. Equally, children who are incredibly shy and easily go unnoticed must not be ignored.Simply recognising that kids might be having a really hard time, giving them space to talk about it with someone skilled, teaching them some resilience and finding a way to work with their parents/carers via the school nurse/social worker could make a lifetime of difference. It is far more important that our kids leave school knowing they are loved, with a real sense of self-esteem and belonging than with good SATS scores or GCSEs. The academic stuff can come later if necessary and we need to get far better at accepting this. A child’s health and wellbeing carries far more importance than any academic outcomes and Ofsted needs to find a way to recognise this officially. In other words, we need to create compassionate schools and try to ensure that school itself does not become an adverse childhood experience for those already living in the midst of trauma.
In North Lancashire, we have created a hub and spoke model to enable schools to be supportive to one another and offer advice when complex safeguarding issues are arising. So, when a teacher knows that they need to get a child some help, they can access timely advice with a real sense of support as they act to ensure a child is safe. These hubs and spokes need to be properly connected to a multidisciplinary team, who can help them act in accordance with best safeguarding practice. This MDT needs to incorporate the police, social services, the local health centre (for whichever member of staff is most appropriate) and the child and adolescent mental health team.
For adults who disclose that they have experienced an ACE, appropriate initial follow up should be offered and a suicide risk assessment should be carried out.
Manage
For children/Young People, the management will depend on the age of the child and must be tailored according to a) the level of risk involved and b) the needs of the child/young person involved. Some of the options include:
In severe cases the child/YP must be removed from the dangerous situation and brought under the care of the state, until it is clear who would be the best person to look after the child/YP
Adopting the whole family into a fostering scenario, to help the parents learn appropriate skills whilst keeping the family together, where possible.
EmBRACE (Sue Irwin) training for safeguarding leads and head teachers in each school, enabling children/YP to learn emotional resilience in the context of difficult circumstances.
Art/play therapy to enable the child to process the difficulties they have been facing.
For adults who disclose that they have experienced ACEs, many will find that simply by talking about them, they are able to process the trauma and find significant healing in this process alone. However, some will need more help, depending on the physical or mental health sequelae of the trauma experienced. Thus may include:
Psychological support in dealing with the physical symptoms of trauma
Targeted psychological therapies, e.g. CBT or EMDR to help with the consequences of things like PTSD (post traumatic stress disorder).
Medication to help alleviate what can be debilitating symptoms, e.g. anti-depressants
Targeted lifestyle changes around relaxation, sleep, eating well and being active
Help with any addictive behaviours, e.g. alcohol, drugs, pornography, food
Recover
Again, this will follow on from whatever management is needed in the ‘healing phase’ to enable more long term recovery. There are many things which may be needed, especially as the process of recovery is not always straightforward. These may include:
The 12 step programme, or something similar in walking free from any addiction.
Revisiting psychological or other therapeutic support
Walking through a process of forgiveness (https://www.youtube.com/watch?v=JQ-j7NuhDEY&list=PLEWM0B0r7I-BXq6_wO4sL0qIwzTWwn_vx&index=9&t=0s, https://www.youtube.com/watch?v=EtexaUCBl5k&list=PLEWM0B0r7I-BXq6_wO4sL0qIwzTWwn_vx&index=9)
We may need to help children go through development phases, which they have missed, at a later stage than usual, e.g. some children will need much more holding, cuddling and eye contact if they have been victims of significant neglect.
Compassionate school environments to help children and young people catch-up on any work missed, in a way they can cope with and reintegrate into the classroom setting where possible, but with head teacher discretion around sitting exams.
To complete the cycle, those who have walked through a journey of recovery are then able, if they would like to, to help others and form part of the growing network of people involved in this holistic approach to how we tackle ACEs in our society.
Hopefully this is a helpful framework to think as widely and holistically as possible. There is much great work going on around ACEs now and we must develop a community of learning and practice as we look to transform society together. We can’t do this alone, but together we can!
The Oxford English Dictionary defines a crisis as:
1 A time of intense difficulty or danger.
‘the current economic crisis’
Mass noun ‘the monarchy was in crisis’
1.1 A time when a difficult or important decision must be made. As modifier ‘the situation has reached crisis point’
1.2 The turning point of a disease when an important change takes place, indicating either recovery or death.
Origin
Late Middle English (denoting the turning point of a disease): medical Latin, from Greek krisis ‘decision’, from krinein ‘decide’. The general sense ‘decisive point’ dates from the early 17th century.
A crisis is still a crisis, even if you see it coming. What is vital, as per Winston Churchill, is that a) we don’t waste this moment, but allow it to be a true tuning point and b) we don’t rush prematurely to actions to try and solve it, but ensure we look deep enough and far enough and then move towards collective steps for an altogether different kind of future.
I think there are some difficult and inconvenient truths that we need to face up to together. If we can do so, then we can move beyond sensational news cycles into co-producing something really exciting. Here are my incomplete thoughts about where we might want to think about starting:
We need to get some perspective! One of the dangers of believing everything is bad is that we start to believe that the NHS is over. It is not over. It is 70 years old and it is transitioning, but it is not over! In the crisis we find ourselves in, let’s remember why the NHS is such an incredible thing and why its integration with social care is so vital. The Commonwealth Fund rates the NHS as the BEST healthcare system in the world, when it comes to equity, care and accessibility. However, our outcomes are significantly worse than that of our peers – there are some really important reasons for this, which we need to understand better. One of the major reasons is that our goals are so short term, that we cannot bring the long term changes to the health and wellbeing that we need – and this is caused by the way the NHS is run and the nature of our political cycles.
We need to stop the boring, binary, partisan nonsense that is the political boxing match. It really is grow-up time when it comes to our arguments. There are some very different perspectives on why we’re in the crisis we’re in, what we might do about it and how we should go about those things. However, shouting our perspectives ever more loudly, whilst never encountering or deeply listening to the other perspectives in the room make it impossible for us to find an effective 3rd way forward together. We are well versed in the blue vs red options, but let us be honest, please. Neither the reds nor the blues are wholly right, and neither is wholly wrong! It is absolutely OK to hold different perspectives, but the manner of our arguments is astoundingly pathetic. Whilst all this shouting goes on, there are several perspectives that are not being heard, important voices, those of the patient, the carer, the poor etc. We need to stop our reactionary, swing left, swing right steering of this great ship (and that’s not to say a centrist approach is best either!) and learn to have some humility. Humility starts with listening and being willing to change. This is being so beautifully demonstrated by the Rose Castle Foundation and Cambridge University through their work with the vastly differing world views of Conservative Islam, Judaism and Christianity and offers us much learning and hope for the NHS and indeed any other of our deeply held belief systems. Anyone willing to have better conversations and find a way forward?
The maths simply doesn’t add up. We need some honesty. A few weeks ago, the head of NHSI Jim Mackey, said that by April the NHS will be in around £2.2billion of debt. That is a very conservative estimate. It is a mathematical impossibility to close wards and scale down the size of our hospitals at a time when district nursing numbers have reduced by 28% over the last 5 years and social care is on its knees AND sort out the deficit! We know what the direction of travel needs to be, but the equation is simply unworkable, due to time and workforce pressures.We need to understand the true scale of the problems we’re facing and be real about how much money is going into health and social care spending compared to what is actually needed.
The reason for this is that health and social care funding is becoming more costly and more complex. Our population is growing in size and people are living longer – this is great, on many levels (although we still need a much better conversation about death and why sometimes we keep people alive, when we could allow them to die well and peacefully). However, as we grow older, we develop more health conditions, and social needs, which require more costly treatments and packages of care, which we’re simply not accounting for, especially when we know the predictions of how our population will grow and age over the next 20 years.
We therefore need to have a long term vision of how we want to build the most safe, excellent, effective, equitable, efficient, compassionate and kind health and social care system in the world whilst recognising in order to so, we will HAVE to make some upfront, BIG investments. It is simply impossible to have double austerity on health and social care and then believe we can do the transformational work necessary for the future change we need. Austerity has woken us up to the fact that there are some inefficient ways of working and some things we could definitely do more effectively in partnership. We’ve learnt that now. However, as a philosophy it is now defunct for where we need to go.
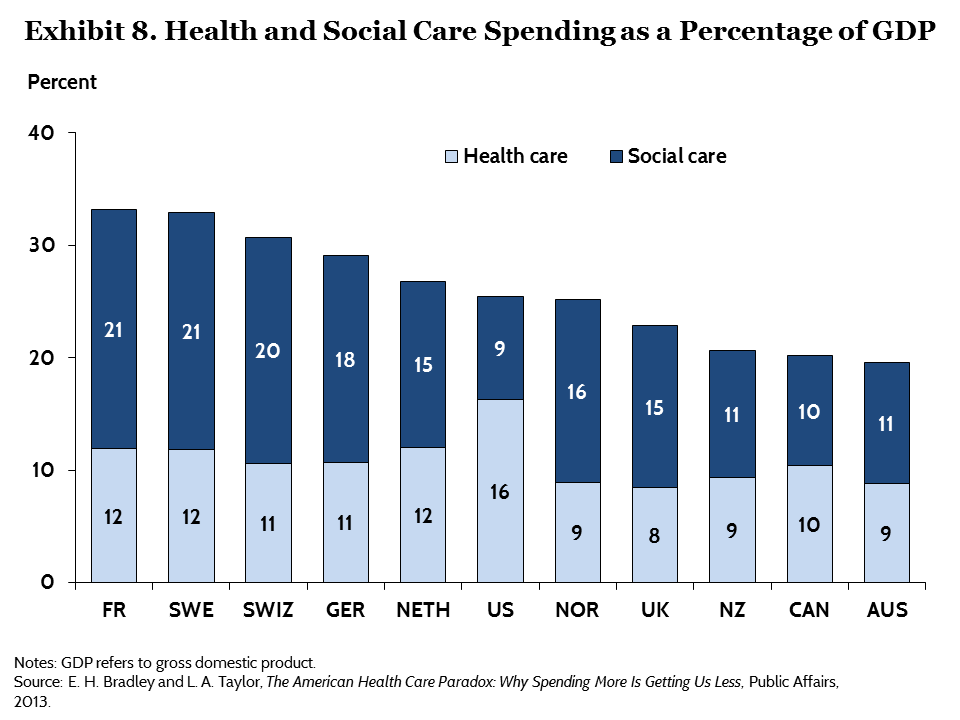
This means, we have to put significantly more money into the system now. Once we have done some more work on the vision and plans for the future (the 5 year forward view is too short and although sets us up a good trajectory, is not ambitious enough), we need to ensure there is a sufficient injection of cash (not removal of it) to make this possible. So, we have some options available to us. A) We could increase tax for everyone – something that 67% of our population seem to be willing to pay. B) We could close tax loopholes and ensure that companies like Amazon and Google pay the tax that is owed. C) We could also increase our GDP % spend on health and social care – remember, currently, we have one of the lowest % spend of any of the other OECD nations. Perhaps a combination of all of these things is necessary.
Creating long term health and social care solutions means that we have to put population and public health as the foundation of the system. We know that prevention is better than cure. We know that if we promote health and wellbeing, disease will be far from us. The disinvestment in these areas and the over reliance on a very stretched and struggling community-voluntary-faith sector is a recipe for disaster. There is huge work to be done in deeply listening to and working with our communities to improve the health and wellbeing of everyone, using the best research, evidence and data available to us through our public health bodies in order to make this shift.
This means we need to continue to tackle the wider determinants of health and think radically about these things as being serious public health issues. This is how the city of Glasgow has gone about tackling knife crime and London has much to learn. We need to apply wisdom and learning to things like smoking, sugar, alcohol, pollution, drugs, road traffic accidents, domestic violence, suicide and adverse childhood experiences. We also need to develop a radically generous philosophy to the areas of job creation, housing, land rights and the care of the environment of which we are stewards not lords.
We have to take greater responsibility and care of the health and wellbeing of ourselves and of those around us. It is not possible for us to have a national health and social care system that is sustainable if we think we can live exactly how we want whilst thinking someone else will simply mop up the mess or pay the tab. Our sugar, food and alcohol consumption, lack of exercise, driving, smoking and drug habits are all areas where we do have to take greater responsibility. NHS staff need to lead by example here. They are also areas where government give those lobbies far too much power and where we need better legislation to help bring about change. It is a both/and not an either/or approach.
We need to create a much more shared-care approach with patients, co-partner with patients to enable them to understand the conditions they live with so that they are able to self-manage/self-care more effectively and create community support groups.
We need to use digital solutions to full effect. We need to widen the access to patients having their own online records, the sharing of data across the system and getting savvy with better apps and technology for the benefit of patients and communities.
We need to change our expectations of what we believe our ‘rights’ are in terms of health and social care. As an example, people phone up a GP surgery and want to see a GP. But there are MANY other allied health and social care professionals who may be better placed to sort out the problem. However, a recent survey in Gosport showed that of the people who phoned up wanting to see their GP, only 9% of them actually needed to see their GP and the rest would have been dealt with more effectively by someone else. We need to get used to the fact that we don’t have enough GPs available for everyone to be able to see one every time they would like to, but there are other professionals who are equally able to help. Another example is that everyone wants to safeguard their local hospital and we tend to have a fixed belief that being in hospital when we’re ill is the best place for us. Actually, especially when we’re older we can receive just as good care at home or in a nursing home and being admitted to hospital adds very little benefit. However, in order to have smaller and therefore more affordable hospitals, we really do have to ensure we have the necessary infrastructure and staffing around community nursing, social care and General Practice. Currently this is not the case and it takes time and investment to grow this workforce.
We need ensure we are training and recruiting the right skill mix of people for the right jobs. This means we need to think at least 20 years ahead with the predictive statistics we have available to us and do some proper workforce planning. We’re are far too short sighted. This will take financial investment now, as stated above, but if we get it right, will leave us with a far more effective and efficient living system in the future.
Our medical, nursing and therapeutic school curriculums therefore need to ensure they are training students for the kind of future we need. We need a complete redesign of some of the curriculums and we need to change the way training is done. As part of this, we need to ensure we are raising good human beings, not just good professionals, with values, culture and great communication skills built into all of the process.
We have to redesign the contracts, as unfortunately without this, some of the behaviour changes simply will not happen. The current contracts across health and social care are the very antithesis of what is needed. This will take some bravery and leadership, but it is time to grasp this nettle. Without this, we will behave perversely because the incentives driving the system and the nature of competition laws are detrimental to the collaborative future we need.
We can only do all of this together. This means our staring place in all of this is to own up to the fact that in all of the above, we simply don’t know. From the place of not knowing, we can ask great questions, bring our bits of expertise to the table and build a jigsaw. There is expertise in national and local government, but certainly not all the answers. There is expertise in the health and social care clinicians, practitioners and managers. There is expertise in our communities and with people who have lived experience of the various complex issues we face. It is only together that we can face the future. Let’s break out of our camps, our deeply entrenched belief systems and find a new way of dancing together. The future belongs to us all. Together we can.
Last week, I had the privilege of being at Morecambe Bay Community Primary School. The school is a beacon of hope in this area. I found it extremely moving to walk round, with Siobhan Collingwood, the visionary and big-hearted headteacher and see the incredible love displayed by all staff towards the amazing children there. It made me realise again how centrally driven targets often make no sense for so many of our children and communities, especially when the base from which they start is so very different. Siobhan and her team are doing the most incredible job at caring holistically for the children here, dealing with complex behavioural issues with such kindness and brilliance that it brings tears to my eyes, even writing about it. Not only so, but the standard of teaching to then try and help these kids come up to the ‘required standards’, being creative with the resources available, is nothing short of miraculous. I would defy any school inspector to rate this school as anything else than ‘outstanding’.
Siobhan and I had a great discussion about the need for health, social care, the voluntary and faith sector, the police and education to work more closely together for the wellbeing of children and young people in our communities. This is already happening in part, through our health and wellbeing partnership and ‘better care together’, but there is far more we can do. We thought about what it might be like if we parachuted fresh into the community now and had to start from scratch, what we might do together…….
We would start with stories – we already have many, from the conversations we’ve had in the community, but we want to really listen and be changed by the responses that we hear. We’re so grateful for the work of the ‘poverty truth commission’, helping us to do just that. We would also definitely pool our resources and prioritise key services that would not be taken away once the community begins to thrive, such as parenting classes, cooking lessons, early support services, a radically caring housing sector, preventative policing strategies (now emerging powerfully in partnership with our town and city councils), social care, mental health champions (something Siobhan has already been part of recruiting 150 locally!), children’s centres and adult education centres as a starter for 10. We would overlay this with the things that are working now – there is so much goodness happening and we don’t negate this. We want to ensure that we could see the health inequality gaps close.
In order to build on this idea of ‘healthy schools’, we would see kids being active every day – despite, limited grounds space, this school, like many others locally are running a mile a day. There is a great scheme here in which all the kids are learning to cook healthy, nutritious food, building vital life skills needed now and in the future. The breakfast and after school clubs are providing many healthy meals each day for the kids and throughout the summer holidays the schools cook – another woman with an incredibly big heart, opens the hall to feed families, who cannot afford to eat during the long breaks. A huge amount of work is being done around gender equality (have you seen the amazing documentary series “No more boys and girls: can our kids go gender free?” On BBCiplayer?). Kids are also given a huge dose of self esteem and know that they are loved and belong. If only the same level of caring support could be afforded through the transition to high school…..
Over the coming months, we hope to co-host some conversations with the community, not on our terms but shaped together with them. Siobhan spent years trying to think of great ideas to get the parents to come into school and interact with her. It wasn’t until the parents set up their own coffee morning in the old garage of the school playground, that she went to meet with them on their terms and started to build some staggeringly life-changing relationships. We know we are changed every time these kind of conversations happen and it blows our world view up so that we can collaborate effectively and co-design services with them. We want to share data with them about health and educational outcomes in order to create a passion for change and do some appreciative enquiry about all the great stuff already embedded in the community. Through these conversations, we want to connect people together and see a social movement for positive change.
The future of Morecambe is bright and full of hope. The communities are strong, the place is beautiful and the people are amazing. Siobhan is just one of many incredible headteachers in this area, committed to one another and this geography through bonds of friendship. If a genuine partnership between health and education can develop here (and it’s part of my vision and ambition to see this done) then who knows what might be possible over the coming months and years?
It is time for Morecambe to find its joy again. It has been the joke for too long, but soon it will become the place where the joke is found and everyone will want to know what we’re laughing about.
I am increasingly concerned by the use of the word “customer” to describe people who use the NHS and social services. I hear it often in meetings and it is, in my opinion really dangerous. It is dangerous for 2 reasons: firstly, it assumes that people “buy” services, which they do not (because our services are not and must not become based upon ability to pay); and secondly it creates a very unhelpful understanding of how we expect people to behave in relation to their own health and the health service i.e. as consumers, rather than participants.
I heard recently about a practice in Columbus, Ohio, in which before beginning an operation, each member of the team: the patient, the surgeon, the anaesthetist the nurse, the ODA and the recovery nurse all stand in a circle and agree who is responsible for which bits of the healing process. It takes into account the ‘checklist’ idea of Atul Gawande and expands it further. Each person, including the patient (except in emergency settings when they are unconscious) have some responsibility to take for the healing that is about to ensue. It is vital that the patient themself understands that they have a key role to play in their own recovery.
If people think of themselves as the ‘customer’ or we think of them that way, we can all too easliy exclude them from taking an active part in their own health journey. The NHS is not a sweet shop or a passive experience in which you have things done to you – at least it shouldn’t be. Creating a ‘customer base’ is the antithesis of a social movement for health and wellbeing and we need to stop this really unhelpful language now!
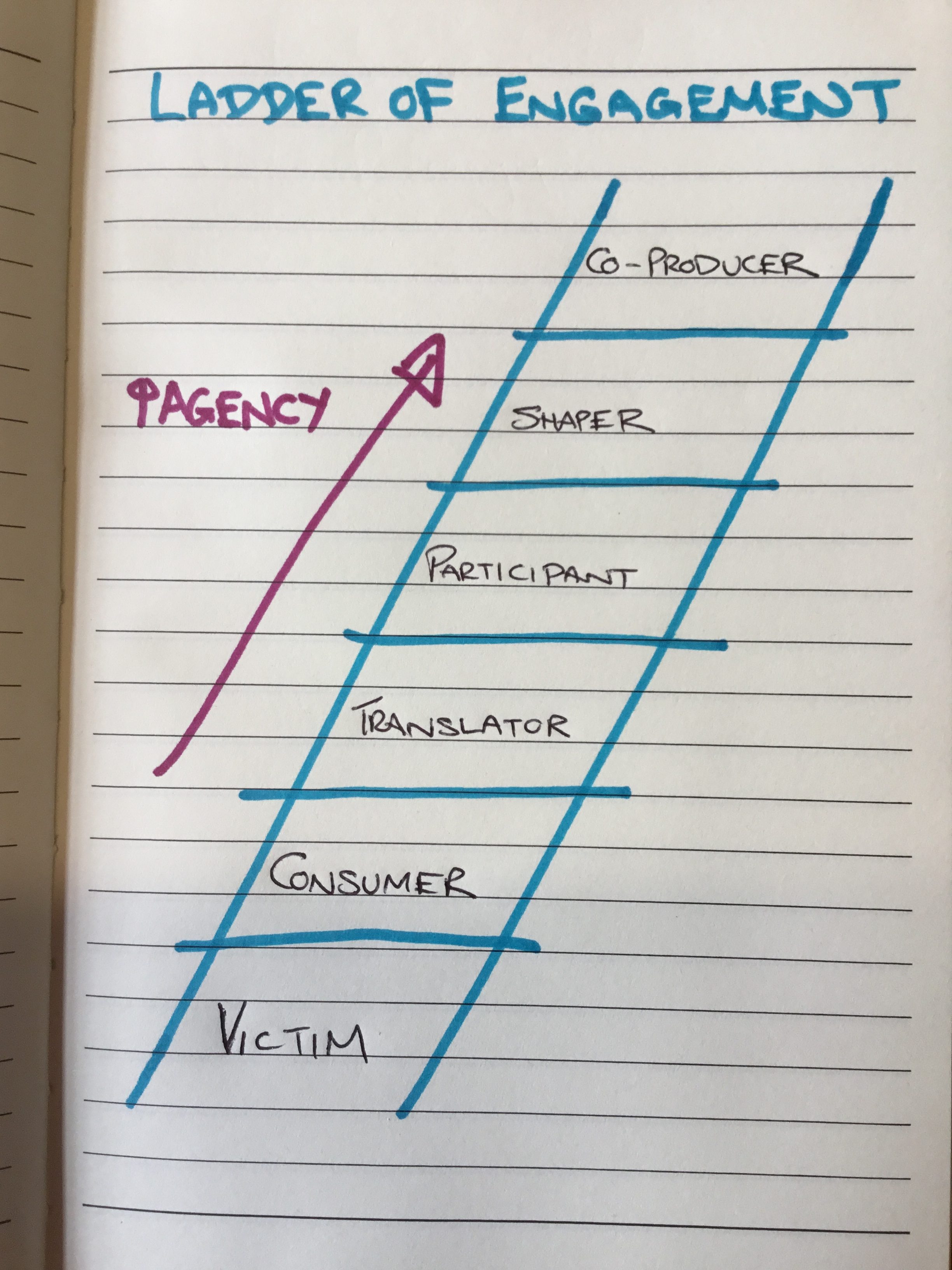
There is a step-ladder approach to thinking about engagement and participation which is really helpful. I’m not exactly sure who first drew this, so can’t give credit where it is due:
We are actively producing and encouraging a society of passivity and consumerism and we need a sizmic shift in our thinking to create a totally different approach to how we think about our health and wellbeing.
If we think of, or encourage people to think of themselves as customers of our health and social care services (and this applies across the public sector, so this could equally be written about education, the cleanliness of our streets etc) then we assign people to the bottom two rungs of the ladder as victims and consumers. It is no wonder that we are facing some of the issues we are. It has created an incredibly unhelpful and unhealthy power dynamic and has caused an enormous strain on our services.
I’m not talking uncompassionately here. I know that many people have to live with long term conditions that can be utterly debilitating and difficult to cope with on a day to day basis. What I’m talking about here is how we respond to people who live with those complexities every day. We don’t have to treat them as victims, nor as consumers. Surely, we want people at least to be able to translate what their choices are – what’s possible for me or even what is in this for me? It would be one step better for people to be able to actively participate in their own care – this can be both active and reflective. But what about people being able to shape or co-produce the kind of care they would like to see and what might their role be in this?
Co-production calls for a double accountability. What is the responsibility of the person who has a certain condition and what is the response ability of the service to work with that person or group of people around that condition/situation? It is not for us to be taking power away from people. We have to learn to work differently and to work with people.
People using the NHS and Social Services are not customers and we must stop talking about them in this way. They are active participants in their own health and social needs, who should be able to shape and co-produce the kind of services we all need to improve our health and wellbeing. This kind of approach is vital if we want to see an end of the consumer mentality and an embracing of a greater sense of corporate responsibility.
That is why I am so passionate that we take our financial difficulties and conundrums out to community conversation. It is not for those of us in positions of power to make decisions on behalf of our communities, (even though this is our statutory responsibility) because if we do, we will only deepen the victim/consumer mentality. No, we must be honest, change our language, share our problems and engage together to recognise that the future of the NHS and Social Care belongs to us all and is our shared responsibility.
The Well is an extraordinary community of people. I respect them deeply and learn so much from every time I have the privilege of being with them, listening to their stories. They are all people on the journey of recovery from drug and/or alcohol addiction. They are welcoming, non-judgmental, caring, embracing and kind. Most importantly of all, they offer hope that no matter how far into hell you have been, there is a way out and no matter how badly you have messed up, you are lovable and worthy of a new chance. There are countless stories of those who have gone before, through the “12 steps”, and found transformational grace and and the chance of a new life. The support they give to each other, especially at times of trouble is based on openness, honesty, trust and a genuine love for each other that holds through difficult battles for a better future. Every story I have heard has humbled me, and each time I am with them, I go away changed and filled with fresh hope. I am so grateful that I can now count several members of the community as my friends. I feel we, as the medical community have much to learn from them.
After my last meeting with The Well community, which was in Barrow In Furness, I then spent some time with an excellent Diabetologist, Cathy hay, who is employed by Cumbria Partnership Foundation Trust, but works at Furness General Hospital (another example of how we are breaking down boundaries and working more effectively as part of Better Care Together). I was learning from Cathy about how she and her amazing team are transforming how they care for and work with people who have diabetes. Like me, she believes that hierarchical behaviour gets in the way of building good relationships across teams, playing to each other’s strengths and working effectively with patients. She has worked hard to break down the ‘need’ for consultant follow-up clinics, putting the power back into patients hands. They have had a much more proactive approach at working with patients to really educate them and empower them about their own conditions through the fabulous work of the Diabetes specialist Nurses and Dietitians and a team of Psychologists, lead by Elspeth Desert, who help patients learn how to face up to and cope with physical health issues.
Group programmes (such as DESMOND, DAFNE or the X-PERT courses) enable patients to build supportive relationships with one another and networks form in which patients are rightly able to become the experts in their own conditions, supported by a team of people who they can draw on, as and when needed – determined by the person with the condition. This cuts the need for outpatient appointments drastically and releases the team to work far more effectively. The ‘Walk Away from Diabetes’ programme encourages those with the earliest warning signs to try and avoid lifelong medication altogether through exercise, dietary changes and accountability with one another.
In some ways, the approach is similar to what I have experienced of The Well and it got me thinking about just how transferable this approach could be across health services, in an extremely timely and cost effective way…..(which although sounds potentially a little mercenary is actually really important – we do actually have a responsibility to use the resources we have as well as we can, and our previous models are no longer deliverable, given our financial and staffing pressures, let alone the increased numbers of people accessing services). What if, once people are diagnosed with a long-term condition, we give them the option of a self-directed, learning approach to their condition, in the context of community with others and a supportive network around them? We could save an inordinate number of unnecessary outpatient appointments. It puts people back in charge of their own bodies and conditions, far more empowered to make informed choices and enables care to be available in a more efficient, cost effective and timely manner. Communities of people, facing up to their conditions together, learning together, helping each other, supporting and resourcing each other and finding improved health and wellbeing at every level as a result.
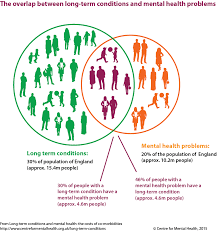
Many people across the UK have at least one long term condition. Many of these people also struggle with a mental health problem at the same time, often linked to the condition they live with. A more cooperative approach can break down some of the barriers and enable people to connect, which will improve both their physical and mental health at the same time.
We are beginning to see an exciting redesign of our respiratory services along these lines, lead by Pat Haslam, Farhan Amin, Tim Gatherall, Shahedal Bari and the team……I wonder how brave we can be across the board and how much better our care might be together if we did?
Here in Morecambe Bay, we are trying to develop a strategy around Population Health – by that we mean we want to take a much broader view of the health needs of those who live in this area, ensuring that we try to tackle the disparities we see in the health of our population. In my opinion this needs a three fold approach.
Firstly, we need to get our own house in order. We know there is work
for us to do as a health system when it comes to ensuring we’re proactive with people’s health. With the resources we have available, we need to ensure that we are treating preventable conditions as well as possible and use the best evidenced-based approach to the care we are delivering. That is why, the excellent Medical Director of UHMB, Dr David Walker, with his vast experiencing in Public Health, is helping us focus on making a significant difference to preventing Strokes (CVAs – Cerebro-Vascular Accidents) across the Bay this year. We are making a concerted effort to ensure that all our patients are getting the necessary pulse checks, blood pressure checks, blood tests and appropriate medications to monitor and manage conditions which can lead to devastating consequences if left untreated or mismanaged. Within this, we are encouraging people to know more about the conditions they live with, understand them and take responsibility to ensure that they are caring for their own health.
Secondly, we are working with people across the Bay to live more healthy lives. We continue to see more and more children running a mile a day and hope that this will soon become the Morecambe Bay Mile, in which it becomes the norm for everyone who lives here to move a mile a day. Our sedentary lifestyles are hugely affecting our health and we’re wanting to encourage all business owners and leaders to ensure that staff have time to be active every day. On top of this we’re starting to work with schools around healthy eating and involved in projects with supermarkets to enable people to make more healthy choices in the face of fierce advertising. We’re also working with high schools around mental health issues and seeing many community initiatives springing up, run by the community for the community, which will improve the wellbeing of all. All of this is backed by our ‘Flourish’ work in our hospitals and ‘Let’s Work Well’ in the community, in which NHS staff are leading by example in changing the way that we work and live.
Thirdly, however, we need to dig deeper. We keep trying to put a sticky plaster over the great pus-filled abscesses that are the leading causes of ill health in our country. Traditionally we have paid much of our attention to dealing with the symptoms of ill health, and whilst thinking about the root causes, we have simply not putting anyway near enough time, energy, or resource into tackling them. The reason for this is two fold: firstly, health and social policy is directed far too much by the political cycle and the short term gains that can proven in small time windows – so we keep tackling symptoms because we can then prove how effective we are!; secondly, in truth, we don’t actually know how to tackle some of the issues and those of us in leadership roles are far too clever and proud to admit that we don’t know how to fix them and that we need to find a new way together, with the communities of which we are a part.
I was having a conversation with Cormac Russell the other day, via twitter, and he gave me this beautiful quote by Ivan Illich: “I believe it is time to state clearly that specific situations and circumstances are “sickening”, rather than that people themselves are sick. The symptoms which modern medicine attempts to treat often have little to do with the condition of our bodies; they are, rather, signals pointing to the disorders and presumptions of modern ways of working, playing and living.”
The reality is that many of the determinants of our health and especially of the health inequalities we see in our society have little to do with the availability or quality of services. No, the biggest factors affecting the health gap in this (and every) area are poverty, housing, loneliness, hopelessness and adverse childhood experiences. If we’re not careful, we end up thinking the real issues are waiting times in the ED, difficulties discharging people from hospital, breaking the 18 week target for hip and knee operations and ensuring there are enough GP appointments at weekends. We must not look at the symptoms and believe that if we tackle these surface issues then we will automatically have better health outcomes for all. Here in the Bay, we are trying to be brave enough to take off the sticky plaster and gaze into the festering wounds in our society, so that we can begin to really do some deep debridement of them and allow real healing to ensue.
That is why my team are focusing on hosting conversations that matter across our communities and seeking to co-create a social movement. Using the ‘Art of Hosting’ we are holding spaces open in which rich conversations can happen. “We don’t just want people to be more healthy and well – many people don’t even know what that means”, as an amazing woman called Gill, from the West End of Morecambe told us recently, “No, we want everyone to be able to experience life to the full, whatever that means for them”. We can’t do this simply by having good clinical strategies – we need something far more holistic and it will involve all of us. We need to start our conversations together with appreciative inquiry. What is already going well? What can we learn from here? Knowing what is good, however, is not enough – we must go further, dig deeper and get to grips with some extremely difficult issues.
When it comes to Poverty, here in Morecambe Bay, we are trying out new economies (like time banking) and having challenging conversations. The Poverty Truth Commission is causing is to really listen to those with lived experience of poverty and learn to co-create and co-commission services, rather than presuming that the ‘experts’ know best.
When it comes to homelessness, inspired by the work in Alberta Canada (https://www.goodnewsnetwork.org/find-out-how-this-canadian-city-has-eliminated-homelessness/) and the Manchester Homelessness Charter (https://charter.streetsupport.net/) – we’re beginning to explore ‘housing first’ for Morecambe Bay, but imagining what it might be like with extra support in place from a caring community like ‘The Well’ in Morecambe and Barrow (https://www.thewellcommunities.co.uk/). I’m so pleased that Dave Higham is provoking this conversation for us here and I’m excited to see where a conversation between those with lived experience of homelessness, poverty and addiction, along with some of us in the public sector, might take us. There’s a challenge to all of us in society – we like the sound of these kind of things, but not in our own backyard….our values must begin to align with our actions. Love without action is not really love.
And what about loneliness and hopelessness? More than ever, we need connection across the generations, turning off our screens and actually being together as humans. In Morecambe we are seeing the launch of the new Morecambe Fringe in September, bringing people together around Comedy and the Arts. More Music are doing incredible work with young people. There are amazing community initiatives right around the Bay. We have loads of festivals connecting people across the district. And what is the role of business here? We need businesses to think abut what kind of enterprise we could see emerge for the youth in our area. Are there more opportunities for mentoring? We have left many of our young people to boredom and with few aspirations. With the help of Stanley’s Youth Centre and the great heart of Yak Patel, we hope to host many conversations with young people to really listen to what it is we could create together to break these problems and build community and hope.
What are we together going to do about the huge issue that is child abuse? We don’t have answers, but we do have questions – and we need to keep asking them. We know that the mental and physical consequences of abuse are utterly devastating and we find it hard to talk about because it affects so many of us. But our interventions are happening too little, too late, and we are missing the vast majority of cases. Our services simply cannot cope with the volume and serious case reviews tell us the same lessons nearly every time. So what? What are we going to do differently? There are definitely things that the public services can do better – but not when our resources are being stripped. What is especially terrible about the cuts to services in our most deprived areas is that ACEs cause poverty, homelessness, isolation and ill health! As a team, we take this really seriously and will be hosting discussions in our schools and local communities about how we raise happy, healthy children. Where is help needed? We’ve become so focused on grades and outcomes in schools…..but do we teach people what to do with their anger? Do we focus enough on values? Are there enough parenting (the hardest job in the world) classes – and if so, are they hitting the mark? What do we need to do differently? We know the situations in which children are more likely to suffer – so what? Have we become so focused on getting people into work that we’ve forgotten just how important parenting is? And if we know that ACE is such a massive issue, are we really making the right choices in terms of what therapies we’re making available for those who have suffered them?
Is it the role of those of us in healthcare to get involved in these discussions? YES! It is the role of all of us in society. Together, we must reimagine the future. We all know that prevention is better than cure, but our short-termism is stopping us from finding the kind of positive solutions that will really make a difference. In face of downward pressure from hierarchical powers, it is tough to make brave decisions to invest in the future, rather than cut our way to balancing the books. But if we really care about the health and wellbeing of our communities, then we have to stop the sticking plaster approach and clean out the gangrenous wounds in our society. We have to deal with the root and not the fruit.






























{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}