I am increasingly concerned by the use of the word “customer” to describe people who use the NHS and social services. I hear it often in meetings and it is, in my opinion really dangerous. It is dangerous for 2 reasons: firstly, it assumes that people “buy” services, which they do not (because our services are not and must not become based upon ability to pay); and secondly it creates a very unhelpful understanding of how we expect people to behave in relation to their own health and the health service i.e. as consumers, rather than participants.
I heard recently about a practice in Columbus, Ohio, in which before beginning an operation, each member of the team: the patient, the surgeon, the anaesthetist the nurse, the ODA and the recovery nurse all stand in a circle and agree who is responsible for which bits of the healing process. It takes into account the ‘checklist’ idea of Atul Gawande and expands it further. Each person, including the patient (except in emergency settings when they are unconscious) have some responsibility to take for the healing that is about to ensue. It is vital that the patient themself understands that they have a key role to play in their own recovery.
If people think of themselves as the ‘customer’ or we think of them that way, we can all too easliy exclude them from taking an active part in their own health journey. The NHS is not a sweet shop or a passive experience in which you have things done to you – at least it shouldn’t be. Creating a ‘customer base’ is the antithesis of a social movement for health and wellbeing and we need to stop this really unhelpful language now!
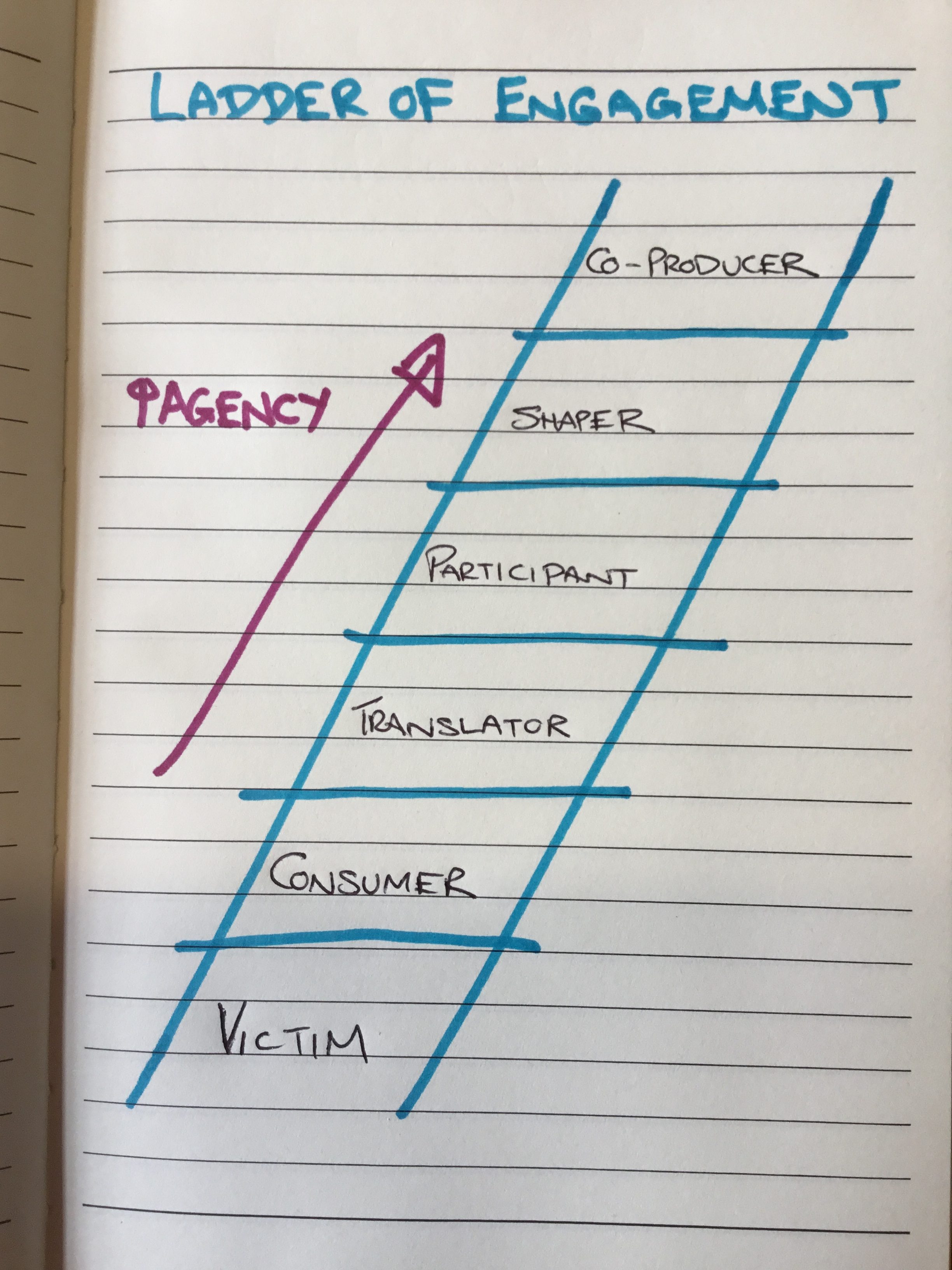
There is a step-ladder approach to thinking about engagement and participation which is really helpful. I’m not exactly sure who first drew this, so can’t give credit where it is due:
We are actively producing and encouraging a society of passivity and consumerism and we need a sizmic shift in our thinking to create a totally different approach to how we think about our health and wellbeing.
If we think of, or encourage people to think of themselves as customers of our health and social care services (and this applies across the public sector, so this could equally be written about education, the cleanliness of our streets etc) then we assign people to the bottom two rungs of the ladder as victims and consumers. It is no wonder that we are facing some of the issues we are. It has created an incredibly unhelpful and unhealthy power dynamic and has caused an enormous strain on our services.
I’m not talking uncompassionately here. I know that many people have to live with long term conditions that can be utterly debilitating and difficult to cope with on a day to day basis. What I’m talking about here is how we respond to people who live with those complexities every day. We don’t have to treat them as victims, nor as consumers. Surely, we want people at least to be able to translate what their choices are – what’s possible for me or even what is in this for me? It would be one step better for people to be able to actively participate in their own care – this can be both active and reflective. But what about people being able to shape or co-produce the kind of care they would like to see and what might their role be in this?
Co-production calls for a double accountability. What is the responsibility of the person who has a certain condition and what is the response ability of the service to work with that person or group of people around that condition/situation? It is not for us to be taking power away from people. We have to learn to work differently and to work with people.
People using the NHS and Social Services are not customers and we must stop talking about them in this way. They are active participants in their own health and social needs, who should be able to shape and co-produce the kind of services we all need to improve our health and wellbeing. This kind of approach is vital if we want to see an end of the consumer mentality and an embracing of a greater sense of corporate responsibility.
That is why I am so passionate that we take our financial difficulties and conundrums out to community conversation. It is not for those of us in positions of power to make decisions on behalf of our communities, (even though this is our statutory responsibility) because if we do, we will only deepen the victim/consumer mentality. No, we must be honest, change our language, share our problems and engage together to recognise that the future of the NHS and Social Care belongs to us all and is our shared responsibility.
The Well is an extraordinary community of people. I respect them deeply and learn so much from every time I have the privilege of being with them, listening to their stories. They are all people on the journey of recovery from drug and/or alcohol addiction. They are welcoming, non-judgmental, caring, embracing and kind. Most importantly of all, they offer hope that no matter how far into hell you have been, there is a way out and no matter how badly you have messed up, you are lovable and worthy of a new chance. There are countless stories of those who have gone before, through the “12 steps”, and found transformational grace and and the chance of a new life. The support they give to each other, especially at times of trouble is based on openness, honesty, trust and a genuine love for each other that holds through difficult battles for a better future. Every story I have heard has humbled me, and each time I am with them, I go away changed and filled with fresh hope. I am so grateful that I can now count several members of the community as my friends. I feel we, as the medical community have much to learn from them.
After my last meeting with The Well community, which was in Barrow In Furness, I then spent some time with an excellent Diabetologist, Cathy hay, who is employed by Cumbria Partnership Foundation Trust, but works at Furness General Hospital (another example of how we are breaking down boundaries and working more effectively as part of Better Care Together). I was learning from Cathy about how she and her amazing team are transforming how they care for and work with people who have diabetes. Like me, she believes that hierarchical behaviour gets in the way of building good relationships across teams, playing to each other’s strengths and working effectively with patients. She has worked hard to break down the ‘need’ for consultant follow-up clinics, putting the power back into patients hands. They have had a much more proactive approach at working with patients to really educate them and empower them about their own conditions through the fabulous work of the Diabetes specialist Nurses and Dietitians and a team of Psychologists, lead by Elspeth Desert, who help patients learn how to face up to and cope with physical health issues.
Group programmes (such as DESMOND, DAFNE or the X-PERT courses) enable patients to build supportive relationships with one another and networks form in which patients are rightly able to become the experts in their own conditions, supported by a team of people who they can draw on, as and when needed – determined by the person with the condition. This cuts the need for outpatient appointments drastically and releases the team to work far more effectively. The ‘Walk Away from Diabetes’ programme encourages those with the earliest warning signs to try and avoid lifelong medication altogether through exercise, dietary changes and accountability with one another.
In some ways, the approach is similar to what I have experienced of The Well and it got me thinking about just how transferable this approach could be across health services, in an extremely timely and cost effective way…..(which although sounds potentially a little mercenary is actually really important – we do actually have a responsibility to use the resources we have as well as we can, and our previous models are no longer deliverable, given our financial and staffing pressures, let alone the increased numbers of people accessing services). What if, once people are diagnosed with a long-term condition, we give them the option of a self-directed, learning approach to their condition, in the context of community with others and a supportive network around them? We could save an inordinate number of unnecessary outpatient appointments. It puts people back in charge of their own bodies and conditions, far more empowered to make informed choices and enables care to be available in a more efficient, cost effective and timely manner. Communities of people, facing up to their conditions together, learning together, helping each other, supporting and resourcing each other and finding improved health and wellbeing at every level as a result.
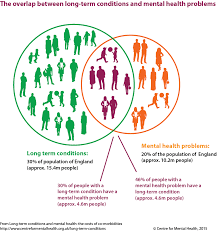
Many people across the UK have at least one long term condition. Many of these people also struggle with a mental health problem at the same time, often linked to the condition they live with. A more cooperative approach can break down some of the barriers and enable people to connect, which will improve both their physical and mental health at the same time.
We are beginning to see an exciting redesign of our respiratory services along these lines, lead by Pat Haslam, Farhan Amin, Tim Gatherall, Shahedal Bari and the team……I wonder how brave we can be across the board and how much better our care might be together if we did?
In my last blog, I was exploring how some of the biggest determinants of our health and wellbeing have very little to do with healthcare at all. They are societal issues, with huge implications on how we live together. Issues like poverty, homelessness, loneliness and adverse childhood experiences are far greater drivers of health inequalities and outcomes than many of the other things we spend an inordinate amount of time and energy focusing on.
However, it is only a social movement of people, willing to face up to and do something about these kind of injustices in our society that is going to bring about real and lasting change. Our old ways of operating, in which public servants try to find the answers and ‘do things’ to communities to ‘fix’ the problems simply are not working. The change we need is only going to come from the grass roots, when communities get together, ask difficult questions, give space for really important discussion and learn to forge new ways ahead in collaboration.
Do we know how to ask good questions? Do we know how to explore complex issues? Do we know how to create the kind of spaces in which we can have really important conversations about the future we might like to co-create together, a future based on values we hold dear, like love, trust and kindness? How much more healthy and well might we all be, if we found a new way of being together, based on collaboration and cooperation? People talk about a new politics – politics is in essence about how people live together, not about how decisions are made in government. A friend and colleague of mine, Ian Dewar, is helping to host a health festival in Lancaster in a few weeks time and he is calling it – ‘The Lost Art of Living’.
The team I work with are committed to training and creating a network of people who would like to co-steward spaces in which we could host these kind of really important conversations. Our hope is that everyone in our area is able to live life more fully, in the best possible health and wellness for them. Here is an example of a training we did in Morecambe in February:
Together, we are are sharpening our skills and using these techniques in a variety of ways to help build this social movement for change in our health and wellbeing. Here are some more ways we are using it:
We are creating a community of practice, unashamedly using these techniques to help shape the cultures of our own organisations and communities and hope to further spread this practice as a method of holding space for new ideas to emerge. Taking time to connect as human beings, asking good questions and using techniques that can really help explore the issues at hand can be truly transformational. the ‘Art of Hosting’ is not a social movement in and of itself, but it helps give the tools and prepare the ground in which one can emerge and flourish. If you live in the Bay, come and co-create with us……if you don’t why not be a catalyst for change where you are?
In the months ahead, we will be offering more training and hosting conversations such as: how do we raise happy, healthy children? How do we live well? How do we work well? How do we age well? How do we die with dignity? Come and be a part of this and let us shape a better future for everyone.
Here in Morecambe Bay, we are trying to develop a strategy around Population Health – by that we mean we want to take a much broader view of the health needs of those who live in this area, ensuring that we try to tackle the disparities we see in the health of our population. In my opinion this needs a three fold approach.
Firstly, we need to get our own house in order. We know there is work
for us to do as a health system when it comes to ensuring we’re proactive with people’s health. With the resources we have available, we need to ensure that we are treating preventable conditions as well as possible and use the best evidenced-based approach to the care we are delivering. That is why, the excellent Medical Director of UHMB, Dr David Walker, with his vast experiencing in Public Health, is helping us focus on making a significant difference to preventing Strokes (CVAs – Cerebro-Vascular Accidents) across the Bay this year. We are making a concerted effort to ensure that all our patients are getting the necessary pulse checks, blood pressure checks, blood tests and appropriate medications to monitor and manage conditions which can lead to devastating consequences if left untreated or mismanaged. Within this, we are encouraging people to know more about the conditions they live with, understand them and take responsibility to ensure that they are caring for their own health.
Secondly, we are working with people across the Bay to live more healthy lives. We continue to see more and more children running a mile a day and hope that this will soon become the Morecambe Bay Mile, in which it becomes the norm for everyone who lives here to move a mile a day. Our sedentary lifestyles are hugely affecting our health and we’re wanting to encourage all business owners and leaders to ensure that staff have time to be active every day. On top of this we’re starting to work with schools around healthy eating and involved in projects with supermarkets to enable people to make more healthy choices in the face of fierce advertising. We’re also working with high schools around mental health issues and seeing many community initiatives springing up, run by the community for the community, which will improve the wellbeing of all. All of this is backed by our ‘Flourish’ work in our hospitals and ‘Let’s Work Well’ in the community, in which NHS staff are leading by example in changing the way that we work and live.
Thirdly, however, we need to dig deeper. We keep trying to put a sticky plaster over the great pus-filled abscesses that are the leading causes of ill health in our country. Traditionally we have paid much of our attention to dealing with the symptoms of ill health, and whilst thinking about the root causes, we have simply not putting anyway near enough time, energy, or resource into tackling them. The reason for this is two fold: firstly, health and social policy is directed far too much by the political cycle and the short term gains that can proven in small time windows – so we keep tackling symptoms because we can then prove how effective we are!; secondly, in truth, we don’t actually know how to tackle some of the issues and those of us in leadership roles are far too clever and proud to admit that we don’t know how to fix them and that we need to find a new way together, with the communities of which we are a part.
I was having a conversation with Cormac Russell the other day, via twitter, and he gave me this beautiful quote by Ivan Illich: “I believe it is time to state clearly that specific situations and circumstances are “sickening”, rather than that people themselves are sick. The symptoms which modern medicine attempts to treat often have little to do with the condition of our bodies; they are, rather, signals pointing to the disorders and presumptions of modern ways of working, playing and living.”
The reality is that many of the determinants of our health and especially of the health inequalities we see in our society have little to do with the availability or quality of services. No, the biggest factors affecting the health gap in this (and every) area are poverty, housing, loneliness, hopelessness and adverse childhood experiences. If we’re not careful, we end up thinking the real issues are waiting times in the ED, difficulties discharging people from hospital, breaking the 18 week target for hip and knee operations and ensuring there are enough GP appointments at weekends. We must not look at the symptoms and believe that if we tackle these surface issues then we will automatically have better health outcomes for all. Here in the Bay, we are trying to be brave enough to take off the sticky plaster and gaze into the festering wounds in our society, so that we can begin to really do some deep debridement of them and allow real healing to ensue.
That is why my team are focusing on hosting conversations that matter across our communities and seeking to co-create a social movement. Using the ‘Art of Hosting’ we are holding spaces open in which rich conversations can happen. “We don’t just want people to be more healthy and well – many people don’t even know what that means”, as an amazing woman called Gill, from the West End of Morecambe told us recently, “No, we want everyone to be able to experience life to the full, whatever that means for them”. We can’t do this simply by having good clinical strategies – we need something far more holistic and it will involve all of us. We need to start our conversations together with appreciative inquiry. What is already going well? What can we learn from here? Knowing what is good, however, is not enough – we must go further, dig deeper and get to grips with some extremely difficult issues.
When it comes to Poverty, here in Morecambe Bay, we are trying out new economies (like time banking) and having challenging conversations. The Poverty Truth Commission is causing is to really listen to those with lived experience of poverty and learn to co-create and co-commission services, rather than presuming that the ‘experts’ know best.
When it comes to homelessness, inspired by the work in Alberta Canada (https://www.goodnewsnetwork.org/find-out-how-this-canadian-city-has-eliminated-homelessness/) and the Manchester Homelessness Charter (https://charter.streetsupport.net/) – we’re beginning to explore ‘housing first’ for Morecambe Bay, but imagining what it might be like with extra support in place from a caring community like ‘The Well’ in Morecambe and Barrow (https://www.thewellcommunities.co.uk/). I’m so pleased that Dave Higham is provoking this conversation for us here and I’m excited to see where a conversation between those with lived experience of homelessness, poverty and addiction, along with some of us in the public sector, might take us. There’s a challenge to all of us in society – we like the sound of these kind of things, but not in our own backyard….our values must begin to align with our actions. Love without action is not really love.
And what about loneliness and hopelessness? More than ever, we need connection across the generations, turning off our screens and actually being together as humans. In Morecambe we are seeing the launch of the new Morecambe Fringe in September, bringing people together around Comedy and the Arts. More Music are doing incredible work with young people. There are amazing community initiatives right around the Bay. We have loads of festivals connecting people across the district. And what is the role of business here? We need businesses to think abut what kind of enterprise we could see emerge for the youth in our area. Are there more opportunities for mentoring? We have left many of our young people to boredom and with few aspirations. With the help of Stanley’s Youth Centre and the great heart of Yak Patel, we hope to host many conversations with young people to really listen to what it is we could create together to break these problems and build community and hope.
What are we together going to do about the huge issue that is child abuse? We don’t have answers, but we do have questions – and we need to keep asking them. We know that the mental and physical consequences of abuse are utterly devastating and we find it hard to talk about because it affects so many of us. But our interventions are happening too little, too late, and we are missing the vast majority of cases. Our services simply cannot cope with the volume and serious case reviews tell us the same lessons nearly every time. So what? What are we going to do differently? There are definitely things that the public services can do better – but not when our resources are being stripped. What is especially terrible about the cuts to services in our most deprived areas is that ACEs cause poverty, homelessness, isolation and ill health! As a team, we take this really seriously and will be hosting discussions in our schools and local communities about how we raise happy, healthy children. Where is help needed? We’ve become so focused on grades and outcomes in schools…..but do we teach people what to do with their anger? Do we focus enough on values? Are there enough parenting (the hardest job in the world) classes – and if so, are they hitting the mark? What do we need to do differently? We know the situations in which children are more likely to suffer – so what? Have we become so focused on getting people into work that we’ve forgotten just how important parenting is? And if we know that ACE is such a massive issue, are we really making the right choices in terms of what therapies we’re making available for those who have suffered them?
Is it the role of those of us in healthcare to get involved in these discussions? YES! It is the role of all of us in society. Together, we must reimagine the future. We all know that prevention is better than cure, but our short-termism is stopping us from finding the kind of positive solutions that will really make a difference. In face of downward pressure from hierarchical powers, it is tough to make brave decisions to invest in the future, rather than cut our way to balancing the books. But if we really care about the health and wellbeing of our communities, then we have to stop the sticking plaster approach and clean out the gangrenous wounds in our society. We have to deal with the root and not the fruit.
Learning requires humility. It requires us to accept that we don’t know everything, that we get it wrong sometimes, make mistakes and need to own up to them so that we don’t do the same thing again. Learning is a vital part of all we do in health and social care, if we are to create truly safe, sustainable, compassionate and excellent services. But humility, although vital, is not enough on its own. There are things we need to put in place to ensure our organisations are continually learning, and not only so but that we actually implement our learning and incorporating it into new ways of working so that we change as a result.
The IHI and Allan Frankel have come up with a really helpful and pretty straight forward framework which enables us to do this. It requires 3 basic ingredients:
1) Leadership commitment
2) Individual responsibility
3) A shared learning culture for quality and safety
Leadership is absolutely vital in setting the right structures and support in place for learning to take place. It requires:
-transparency with the public, patients and staff
-vulnerability about weaknesses
-openness about what is being learned and what is changing as a result
-ensuring we are learning with and from our patients not just within our clinically teams. (Some of the most powerful learning we have done in Morecambe Bay has been from women using our maternity services. Our attitudes, communication skills and expertise have all improved dramatically as a result).
-commitment to the psychological safety of staff in developing a culture in which no question is too stupid and no concern is dismissed
-genuine care for each member of staff, creating a culture in which every person can be mentored, coached and encouraged
-time given and protected in which learning can be fostered
Personal Responsibility
Who are you?
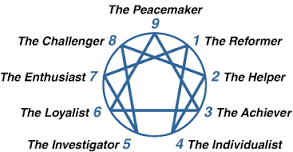
In my role as a coach/mentor or trainer I have found that we have become far too obsessed with ensuring that people have the right skills but not necessarily paying too much attention to who people are, what their character is like, what their strengths and weaknesses are and how they are developing as a human being. Our medical/nursing and other clinical schools are filled with people eager to learn but who often have no idea about who they are and who, not what they would like to become. Knowing who you are as a person, hugely affects your clinical practice and we do not give it any way near enough attention. I am personally a huge fan of the Enneagram. For me it has been transformational to understand as a type 7, not only what my root need is (to avoid pain) what my root struggle is (gluttony) how I do under stress (become a falsely happy control freak) but also, what my invitation is (towards sober joy and deeper understanding), how to become a more healthy version of me and therefore a better gift to my family, my team and all the people I’m trying to serve. It has helped me to recognise when I’m doing well and when I’m not and to understand how to bring my core strengths to the fore whilst also recognising where I need discipline and boundaries to function from a more healed place. We each have a responsibility not just to be good at stuff, but to be good at being us. And being us is more than just knowing how we function (e.g. ENFP in Myers-Briggs) but to get below the surface to the core of what makes us tick, that makes us human. Knowing who we truly are enables us to be better, kinder, more humble, genuine, compassionate people, who put aside the need to beat others down and learn to appreciate them so much more. When you really know the team you are working with, they become your friends, you understand the little idiosyncratic things about them with a whole lot more patience and you can also challenge them when they are not behaving in a way that is conducive to good care and you can also receive that challenge back when you are out of line. I wish that we were more interested in caring about who we are rather than only in what we can do. This has got to be a part of the culture of joy I have blogged about previously.
How are you?
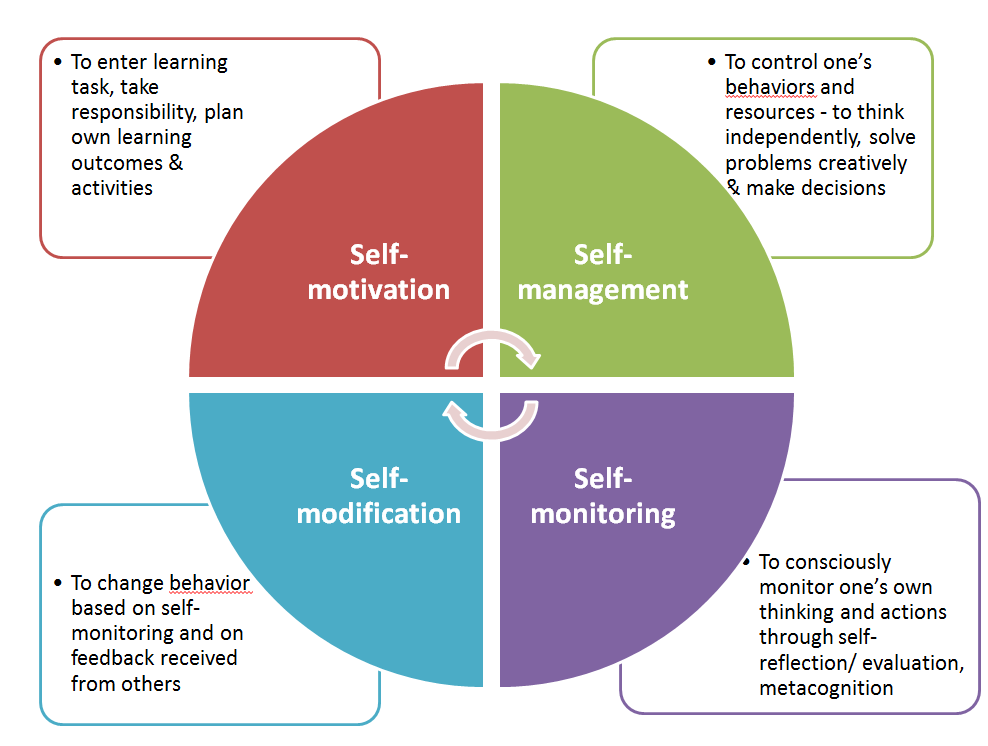
Personal responsibility beckons us to be more honest with ourselves and others about how we’re doing emotionally/physically/mentally. It has been a transformational practice in our team to simply check-in with each other and talk about where we’re at. In this way, we can carry each other when needed and treat each other with kindness and compassion. But our individual agency, must also cause us to recognise when we are at a wall/ceiling/limit personally or professionally. We must simply own up when we don’t know something or are out of our depth or need help. We cannot pretend to be able to have a competency that we don’t have. We need to be self-aware and humble enough to accept when we don’t know something or have become unwell and ensure that we take it upon ourselves to find out or get the help we need. This is learning to have an internal, rather than an external locus of control. An external locus, always looks elsewhere for the answer. An internal locus takes responsibility to find out and keep learning. We need to develop a core value, that learning is really really important and we will prioritise ensuring that we keep making time to do so, through whatever form that takes, especially reflective practice. Yes there is some dependency on supportive structures and time being given, but there is also that sense of motivation that comes from within that we take ourselves and our roles seriously. It’s one of the reasons why I’m such a fan of a combination of problem-based learning and a solutions-focussed approach. If we do this ourselves and foster it in our teams, the care we provide will be beyond stellar!
Why are you Here?
We talk about the law of two feet in our team. You are responsible to know why you are here, or if you need to be somewhere else. That might even mean a job change, but more often than not it means having some good boundaries, knowing whether or not you really need to be at a certain meeting or somewhere else, if you should be doing what you are or if you need to ensure other things get the right focus. And what about yourself? Have you taken time to eat well, stay well hydrated, exercise, sleep well, maintain health in your relationships? In teams that care for each other we need to help each other to know why we are there and why we are important.
A Shared Learning Culture
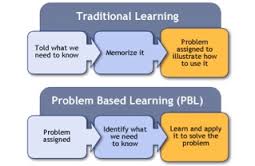
It’s amazing to me that so many of our learning environments are still so teacher-based. Adult education is so much more empowering than this and it’s high time our clinical learning environments (both preclinical and in every day life) reflect this. They should also be more inclusive and we should be learning with and from our patients far more than we do. Although the above graphic applies to classroom settings, it contains many lessons for us.
With leadership and personal agency holding true, a culture then develops in which continuous learning is the norm. Learning environments, fuelled by kenotic power create a space in which an organisation can begin to truly flourish. It creates a net of accountability, teamwork, improvement and measurement, making the entire system more reliable. It is vital that we create this as one of the core principles upon which we build our future health and social care systems.
NHS – we have a problem! This blog forms a hiatus in the middle of a 4 blog mini-series about what I call the four rings of leadership (in the context of healthcare). I have been musing on some statements made at the IHI conference in London, Quality 2017, and before I go any further, I want to take a pause to reflect on the notion of power. Helen Bevan says that the number one issue facing our health care system is the issue of power. I would suggest that unless we seriously reflect on power and how it manifests itself in our systems and in us as individuals, then we will never be able to co-create health and well-being in our society.
In my last blog, I mentioned an excellent talk that I heard Derek Feeley of IHI and Jason Leitch, the CMO of Scotland, give together about our need to “cede” power, if we are to build safe, high quality, economically sustainable health systems. They contend that we need to move from keeping power, to sharing power and then ceding power. To cede power, means to transfer/surrender/concede/allow or yield power to others. I do believe this is correct. I believe that true leadership is absolutely about being able to ’empty out’ positions or seats of power, so that all are empowered to effect positive change and build a society of positive peace. However, my contention is this: ceding power is not helpful unless we first deal with the very nature of power. Once we have dealt with its very substance can we truly cede it through our organisations and systems to bring increased well-being for all.
I have talked many times over the dinner table with my great friends Roger and Sue Mitchell about the nature of sovereignty and power. Sovereignty is a dominant theme within our political discourse at the moment, at a national and international level. It is worth reflecting that sovereignty (the right to self-govern) is utterly intertwined with our understanding of power, and we need to pull the two apart if we are ever to cede the kind of power that can transform the future. If we do not recognise (have a full awareness/deeply know) this, we will continue to inadvertently create hierarchical dominance and systems that become the antithesis of what they are created to be.
We see the issue of sovereign power at work every day in the NHS. We see it in terms of power edicts from on high, without understanding the local context or issues worked through in a relational way. We see it in the way these edicts are then outworked through leadership and management styles, which are very top-down and hierarchical in nature, eating up people like bread in the process – what Foucault calls “Biopower”. We see it in the way wards are managed and in the way GP surgeries are run. Sovereign power says “I’m in charge around here” and “we’re going to do things my way”. We see it in individuals who choose to practice autonomously without thinking about the wider implications on the system, prescribing however they would like to, without thinking about the cost implications. We see it in the attitude of some patients, when it becomes about “my rights” with an unbearable or unaffordable pressure put onto the system. If we multiply sovereign power, we simply end up with lots of kings and queens who defend their own castle, creating more barriers, walls and division in the process. Sovereign power is defunct and dangerous and it is this which is currently destroying our ecosystems and wider society. The “I did it my way” approach is rooted in self preservation and ambition and does nothing to help us build health and well-being in society. Sovereign power stands in the way the very social movements we need to see, because Sovereign power is based on fear.
Sovereign power has its roots in certain streams of theology and philosophy which have in turn laid the foundation for a way of doing politics and economics based on the supremacy of the state and within that the individual. However, the damaging effects of this are seen on our environment and on community, with utterly staggering levels of inequality, injustice and damage to the world in which we live.
If we are to truly cede a power that is effectual in changing the world, then it is not enough to simply reconfigure (rearrange) it, or reconstitute it ( i.e. give it a new structure/share it). First of all, we must revoke it! In other words, we must look ‘Sovereign power’ straight in the eyes and reject it, cancelling it’s toxic effects on our own selves and on that of others. We must change our minds about it and embrace instead a wholly different kind of power. Sovereign power has not changed the world for the better so far, and I hold no hope of it doing so in the future. No, we don’t need Sovereign power and we certainly don’t want to cede it. Instead, we need kenotic power. Kenotic power is based in self-giving, others empowering love (Thomas Jay Oord). It empowers others, not to live like mini-dictators, but to also dance to a very different beat.
I used to play the card game bridge, with my Grandpa (he was an amazing man, who invented Fairy Liquid!). In bridge, to revoke something is to fail to follow suit, despite being able to do so. Kenotic power refuses to play the game of Sovereign power. It embraces an entirely different approach. And as many through the ages have found, this kind of power is truly costly, and can even cost you your career or life; but it is the only kind of power that truly changes the world for good. Jesus, Rosa Parks, Emmeline Pankhurst, Gandhi, MLK, Malala Yousafzai, Nelson Mandela, Florence Nightingale and Mother Theresa are just some, who have embraced this ‘self-giving, others empowering love-based power.’ This is the kind of power we need now. We need it in healthcare and in every other part of our society.
Kenotic power is vulnerable but it is not about being a door mat. It is like a beautiful martial art, in which we can say “I won’t fight you and you can’t knock me down, unless I let you” In other words, we lay down our rights and power freely, they are not taken from us by force. So, even when energetic attacks are launched against us, this kind of power allows us to move out of the way, allow the attack to pass through and then to come along side the person and help them see another point of view. Switching to this kind of power is far more creative, less combative and far more fruitful in creating a way ahead full of possibilities without the need for making enemies in the process. We must challenge the deep structural belief that our political and economic systems must be built on and can only be held together by Sovereign power. What if we developed systems based on love, trust, joy and kindness, aiming for the peace and wellbeing of all (including the environment?) – what might such a health system be like? It will take a social movement for us to get this shift, and as I wrote in my previous blog: You might call this a re-humanisation of our systems based on love, trust and the hope of a positive peace for all. But this social movement is not aiming for some kind of hippy experience in which we are all sat round camp fires, singing kum-ba-yah! This social movement is looking to cause our communities to flourish with a sense of health and wellbeing, to have a health and social care movement that is safe, sustainable, socially just and truly excellent, serving the needs of the wider community to grow stronger with individuals learning, growing and developing in their capacity to live well.
I agree wholeheartedly that the most important role of leaders is to cede their power, so that all can truly flourish, where there is a far greater sense of cooperative and collaborative agency within our (health) systems. But if we do not examine the nature of this power, we will only perpetuate our problems.
Martin Luther-King said these famous words – they are seriously worthy of our reflection:
“Power without love is reckless and abusive and love without power is sentimental and anaemic. Power at its best is love implementing justice, and justice at its best is power correcting everything that stands against love.”
As the crisis in the Western World deepens, and the growing reality sets in that business as usual simply can no longer continue nor solve our problems, our systems must change the way they view, deal with and hold onto power. The NHS is no exception. If we want a health and social care system that is of the highest quality, safe, sustainable and economically viable for the future, we need to understand the power of social movements, both within our systems and through the wider society. This is something we are really committed to in Morecambe Bay and so it was with great delight that I listened to the excellent Helen Bevan, talk about just how vital social movements are for the NHS and healthcare, worldwide at the recent IHI conference in London, Quality 2017. This blog will be an amalgamation of what Helen shared and my own thoughts about our early experiences with social movements.
A social movement in health and social care involves us all learning to connect, collaborate, cooperate, cocreate and coproduce at a level we have never done so, until now. But our circumstances are forcing us to reconsider the ways in which we work. We need the creative substance that is within our teams to be heard and harnessed so that we cut our waste and work more effectively together. The issues we face, need facing by us all, together; not by some board in an isolated room, making decisions based on diktats from on high, on behalf of us all. But even this will not be enough. Those of us stuck in the system have become too homogenized in our thinking for us to do this exclusively from within. We need our citizens to help us re-imagine what it means for us to be healthy and well. We must stop designing things for our communities or doing things to them, instead we must design and do things with them. We must analyse, create and enact together and to do this, we must learn to solve the issues of power.
Helen Bevan, with her background in social science, demonstrates the great debate about the interplay between our organisational structures (rules) and agency (freedom) when it comes to effecting change. Where does the “permission” come from to enact the change we need to see? Is it externally generated by those in positions of power, or is it internally generated by a personal motivation? Our experience in Carnforth and Morecambe in community conversations has been a bit of both. There are many people of incredible heart and goodness, waiting to do something new and good that will positively affect the health and wellbeing of society, but are perhaps waiting for that sense of community backing, support, encouragement or indeed permission. With a bit of coaching or spurring on, we have seen some amazing initiatives begin that are bringing transformational work into our area and causing us all think differently. We need both individual agency AND corporate agency. Helen describes individual agency as being when people get more power and control in their lives – we see this in patient activation, shared-decision making and self-care – a greater sense of autonomy and responsibility. Collective agency, on the other hand, is where we see people act together, united by a common cause, harnessing the power and influence of the group whilst building mutual trust.
We have seen this used powerfully, in just one example by our maternity liaison service committee, who together have challenged our system to think more carefully about how we communicate to women, especially at key or stressful moments of their obstetric care. These stories are now a compulsory part of training for all who work in our maternity service and have significantly improved both our skill mix and ability to provide excellent care.
What is absolutely vital to understand is that we do not become transformed alone. We are transformed when we are in relationship with others (Hahrie Han). The problem is that we don’t really encounter the “other” enough to be changed. However, when we let go of the kind of power that is held by the few, pushes others down, uses command and control, that is closed and transactional, and instead embrace a power that is held by the many, shared, open and relational, then we can begin to see the change we need (Hirschman and Ganz).
David Holzmer says that we are witnessing the collapse of expertise and the rise of collaborative sense-making. I would suggest that this has been going on for some time, but our systems have been incredibly slow at catching onto the change around us.
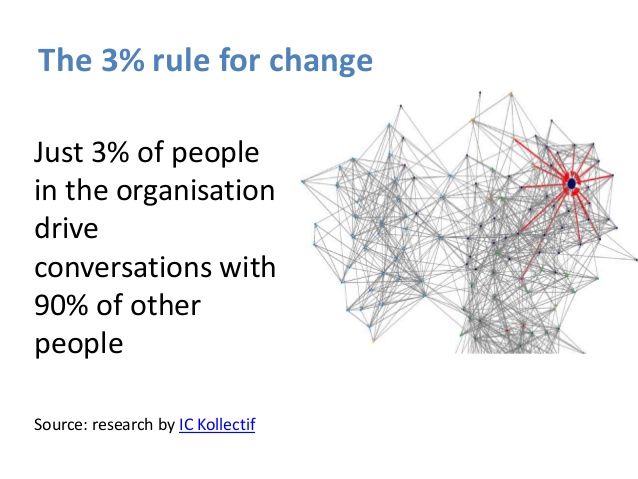
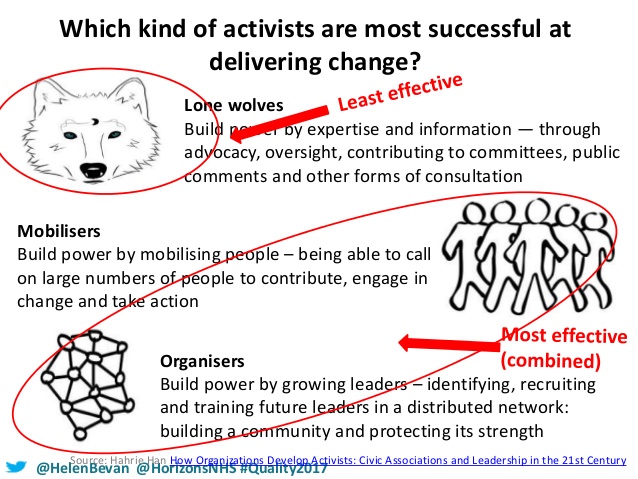
Now, what is hugely encouraging is this: research by Kollectif shows that you only need 3% of people in an organisation/society to drive the conversations with 90% of other people. In other words, you don’t have to get everyone on board from the word go. You find your passionate people with a sense of agency, infect them with the virus and watch it spread. These people need to be a mixture of ‘lone wolves’, mobilisers and organisers. Lone wolves are people who have been trying to help change happen for a long time but can sometimes feel like an annoyance to the system, so they are given tokenistic positions, patted on the head and patronised into exhaustion. Mobilisers build power by calling large numbers of people to contribute, engage in change and take action. Organisers build power by growing leaders in a distributed network, building a community and protecting its strength. We need all of them, though mobilisers and organisers will be the most effective in creating agency and bringing about lasting change (Hahrie Han).
Joe Simpson says that ” great social movements get their energy by growing a distributed leadership.” The cult of celebrity can be powerful, but is not effective. The beautiful thing about a social movement is that is depends not on money, materials and technology but on relationships, commitment and community, and as the movement grows, these resources increase, rather than diminish. The problem, as Don Berwick puts it, is that leaders in position of strategic influence, are simply not seeing the resources available to the biggest problems we are facing.
Jason Leitch and Derek Feeley have powerfully shown that performance management (keeping the power), based on targets, sanctions and inspections can only get us so far. Quality improvement (sharing the power) gets us a little further, but mobilising social action, or co-production (ceding power) has a far greater potential to bring lasting change and far better outcomes for all.
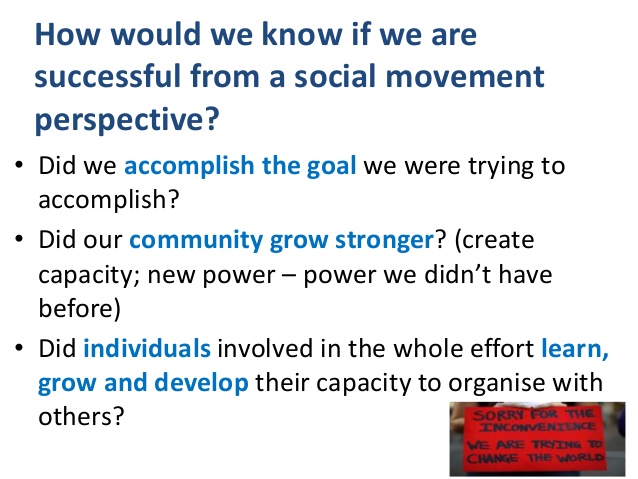
So, how do we catalyze a social movement and how would we know if the movement was being “successful”? Well, our experience in Morecambe Bay is that you start with the 3%. You start with those who are drawn to the conversation, who recognise the need for change and who want to be part of it. You start with transparency, with openness, honesty and vulnerability about the mess we find ourselves in and the truth that we no longer have what it takes to solve the problem. And you start with really good questions and then deeply listen to the conversation which is emerging so that we ourselves are changed and can therefore be part of the emergence of something new, which operates on an entirely different kind of power.
You might call this a re-humanisation of our systems based on love, trust and the hope of a positive peace for all. But this social movement is not aiming for some kind of hippy experience in which we are all sat round camp fires, singing kum-ba-yah! This social movement is looking to cause our communities to flourish with a sense of health and wellbeing, to have a health and social care movement that is safe, sustainable, socially just and truly excellent, serving the needs of the wider community to grow stronger with individuals learning, growing and developing in their capacity to live well. That is what we must measure!
And so we need disruptive co-creation, which breaks through the top-town/bottom-up approach and causes us to see and hear like we have never done before. It is hugely exciting and enables managers to stop feeling like they have to extract as much performance as possible from the system, flogging the workforce, blocking change and innovation and inadvertently driving down the quality of care in the process.
The invitation is instead to become part of the change that we all long for. If we’re going to have an NHS in the future, we have to give it back to the people and work with them. In order to do this, we have to deal with and change our relationship with the very notion of power – something I will turn my attention to on the next blog!
A Culture of Joy is the biggest determinant of safe and high quality healthcare! That is such a phenomenal statement that it is worth reading over and over again, making it into a poster, sticking it on your wall and meditating on it morning and night. It feels to be simultaneously absolutely true and somehow beyond belief. I’ve previously blogged here about the need for a culture of kindness in the NHS, and I hold to that – kindness certainly doesn’t exclude joy (!), but a Culture of Joy….. I don’t know, in a day in which 50% of our staff admit to feeling burnt out, can we honestly say we have developed this throughout our health system in the UK? So, what does it take to build this? How do we have a joyful workplace? If it is really the single largest factor affecting patient safety, which research from The Mayo Clinic, The IHI and The Quality Forum tell us it is, then we better sit up, pay attention and do something about it!
There are 3 key ingredients to creating a culture of Joy. The first (and this is in no sense a hierarchical order!) is leadership, the second is how
teams actually function together and the third is personal responsibility. You will see the words incorporated from the ‘culture circle’ in bold!
Good Leadership: Here’s a fascinating fact, I learnt from Stephen Swensen, of The Mayo Clinic – The bigger the signature of a CEO, the worse the outcomes for patients, staff and the finances of the organisation!! CEOs are responsible for setting the structures in place that allow healthy cultures to develop. Leaders create a culture of joy by having humility and developing 5 key behaviours:
Appreciation – good leaders build joy in their teams by saying ‘Thank You’ – it is one of the things the team at my surgery consistently tells us, as partners. Of course we are grateful, but we don’t say it enough. Every member of a team knowing that they have value is so vital. I remember, as a house officer on a medical ward watching a lady called Jean, cleaning the ward and saying hello to all the patients. I went up to her and said, “Jean, I just want to thank you for everything you do on this ward, every day. The way you keep this place clean helps fight off infections and keeps people well; and the smile and kindness you bring is really comforting to people who are scared or hurting.” To my great surprise, she burst out crying. I asked her what was wrong and she told me that she had worked on this ward for 25 years and no-one had ever said ‘Thank You’ to her. My favourite hashtag on twitter is trybeinggrateful – it costs so little.
Transparency – good leaders communicate openly with their teams. They don’t do ‘special huddles’ in which they invite a few ‘high level’ people to know their secrets. No. They communicate with honesty and openness and this builds trust. And with trust they are able to negotiate difficult situations and requests of their teams, because there is a belief that everyone is in it together.
Ideas – They look to their teams for ideas. One of the things I loved learning about recently is that the CEO of Toyota in Derby, deliberately does not park his car in the special ‘CEO parking space’ right next to the building. Instead, he parks it at the far end of the factory, so that the walk to his office takes him through every department, (a good 30 minutes of his time), so he he can say “hi” to his staff, connect with them and ensure that he is hearing about their ideas for innovation and improvement. Toyota takes 2.5 million suggestions from its staff every year. This simply doesn’t happen enough in the NHS, and I wonder how many CEOs take time at the start of the day, to walk the corridors, listen to patient stories, understand the pressures in the ED, hear the heartbeat of the wards and get a sense of the ideas brewing in some of the most compassionate, caring and intelligent staff of any organisation in the UK. If we are to transform the NHS into a system that is truly safe, sustainable and excellent, we must listen more to the ideas of our teams and in doing so, we will cut waste, undo the reems of red tape and instead find we are working far more effectively and efficiently. To embed this into the culture, there must be psychological safety – that means that no question is too stupid, no idea is too dumb and it is safe to bring to attention concerns a person may have, without a fear of retribution. One great question for leaders to ask is, “what are the pebbles in your shoes?’ – in other words, what matters to you? Or what are the barriers for you here? What’s getting in the way? Great CEOs do not have great answers, they are willing to work with complexity and have great questions!
Career Mentorship – every person needs to be able to keep learning and develop in their role. We all need mentors or coaches at different stages in our careers, and ensuring these structures are in place to support staff as the complexity and pressure we deal with increase, is vital in building joy. People who are developing in their role are naturally safer in their role.
Inclusiveness – To a good leader, it doesn’t matter who you are, what you look like, what you believe, what your sexual orientation or status might be. You need to know that you are welcome and you are loved just as you are. Inclusive teams that do not scapegoat, do not sideline and do not bully are joyful teams. Joyful teams celebrate difference and thrive off it.
Joyful Teams: It’s really important to understand that joy does not mean false happiness. It does not mean that we walk around with fake smiles on our faces all the time and pretend that everything is ok. Joy is much deeper than that. We deal with very sad and difficult things in our workplaces every single day. We break bad news, we hold people as they take their final breaths, we watch people make terrible life choices, we see and carry the hurt of those who suffer loss and each of us has our own burdens we carry from the lives we live outside of work. Joyful teams do not pretend like that stuff isn’t happening every day – quite the opposite. Joyful teams develop three key qualities:
Camaraderie. The high school musical song – ‘We’re all in this together’ is a great theme tune for NHS teams. People need to know that they belong, that they are loved and that people care about them. On good days, we celebrate together, on bad days, we pull together. Joyful teams develop encouragement, support and kindness in how they treat each other.
Purpose. Joyful teams have a real sense of shared vision and purpose. They know what they are there to do and each person knows that they are valued in that team. The posh term for this is a sense of corporate agency. This is our job to do, we are responsible for what happens here and we want to do our work with excellence.
Trust. It is really important that individuals feel trusted to do their job without feeling like they are always being watched or criticised or that they have to give an account for every action. When people feel trusted, they actually work more effectively and produce better outcomes.
Personal Responsibility: in order to create a culture of joy, it is not just the responsibility of the CEO or team leader, nor the atmosphere created by the team as a whole – we each have a responsibility to steward and hold to this culture. And that means taking care of our own needs. We need to be active, eat well, take notice, be mindful, sleep well, forgive those who hurt us and have good friendships. Making sure that we ‘host ourselves’ well, ensures that we play our part in building the culture of joy that is so vital to the providing care that is of the highest quality and safety. There is a personal accountability to ourselves and to those we work with to ensure this is so. There is also personal agency that rises to the challenge that each one of us can set a new trend and make a significant difference to the culture in which we work.
In the midst of all we are currently facing in the NHS, for the sake of our patients and their families, it is vital that we build cultures of joy now and cultivate them for the future.
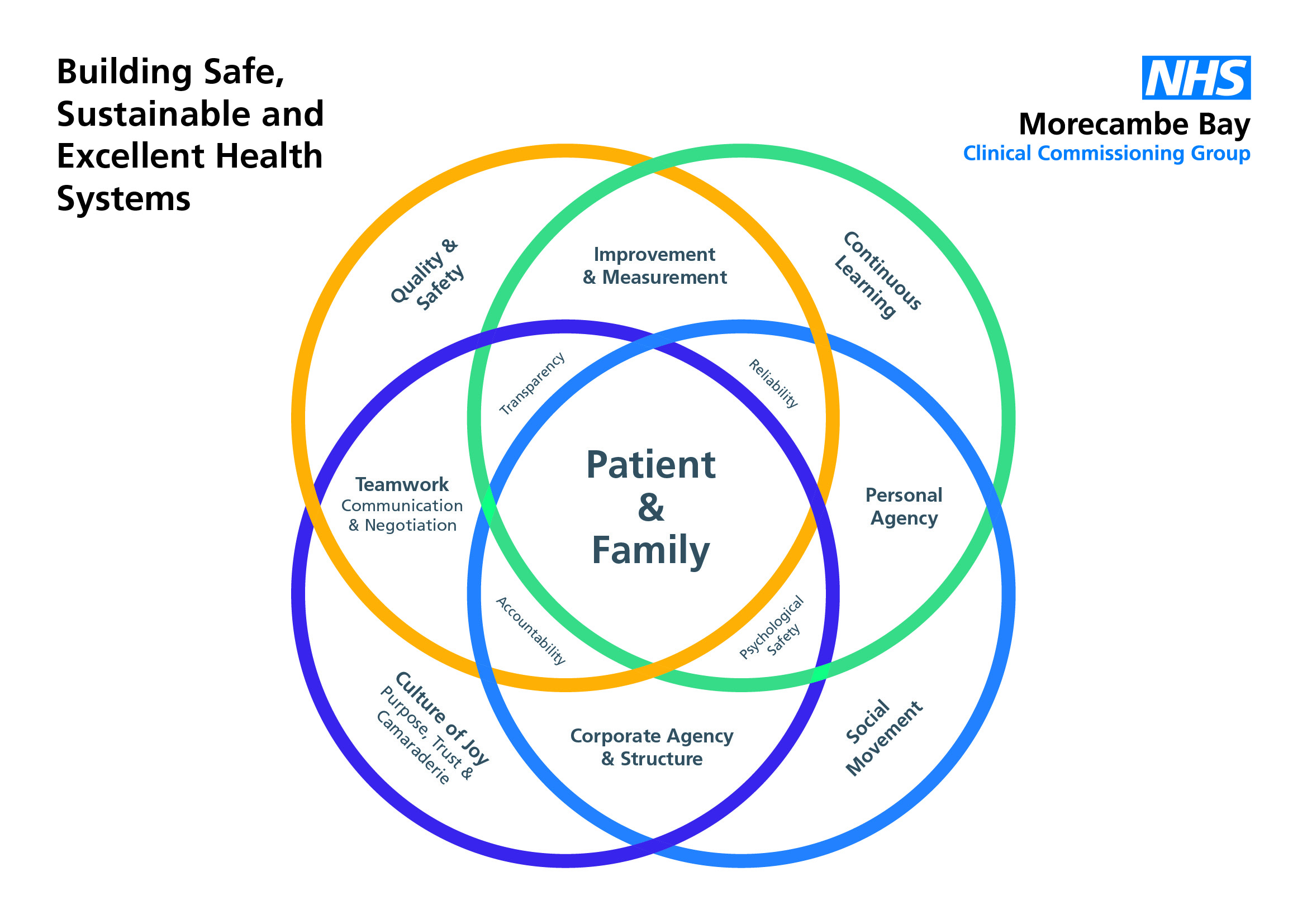
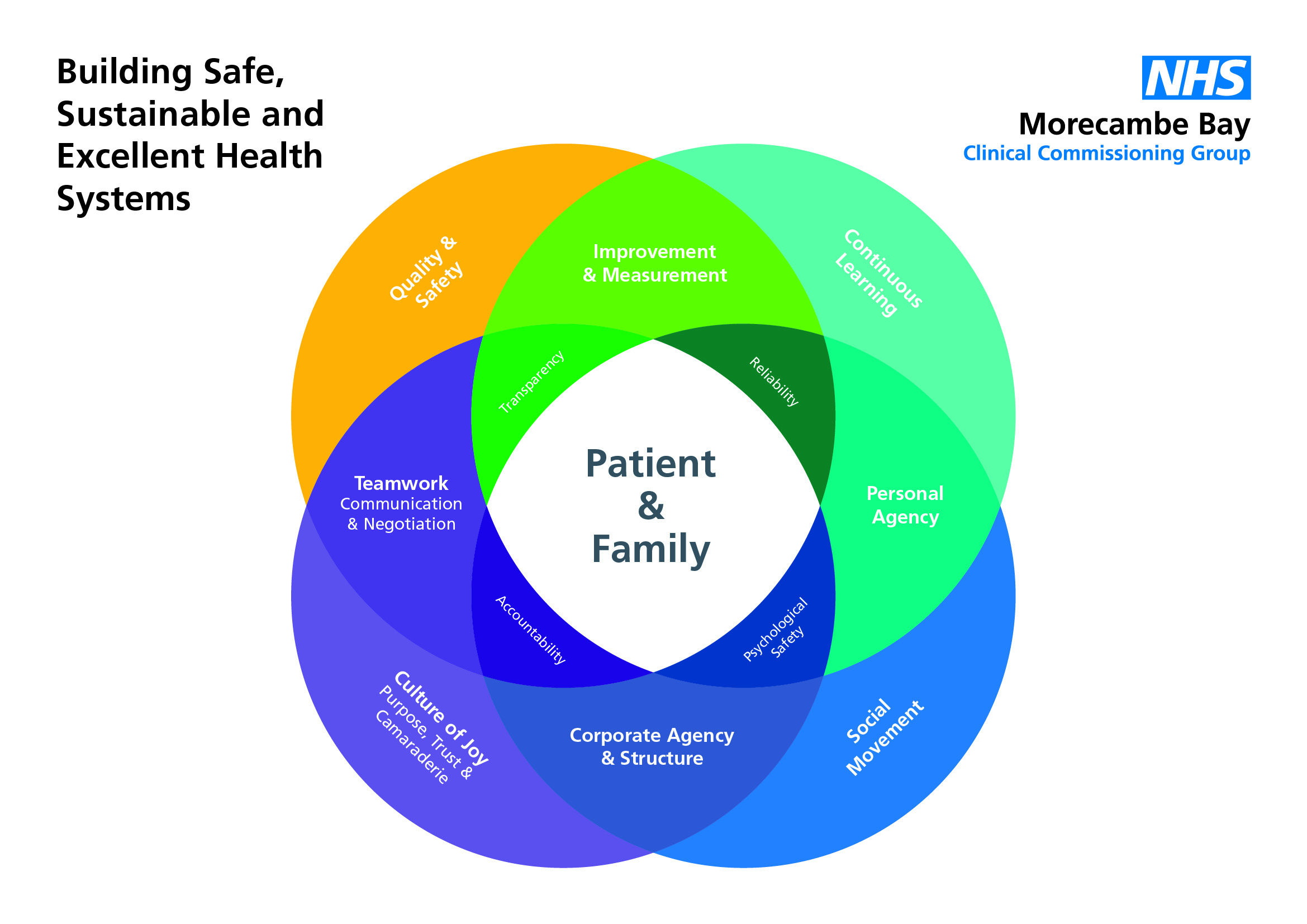
I went to London a couple of weeks ago for the IHI (Institute for Health Innovation) conference in London – Quality Forum 2017. The focus was on Quality and Safety in Healthcare, with some hugely surprising and refreshing perspectives from around the world. It was absolutely great and I learnt loads. I’ve tried to distill my learning from the time into a single sheet diagram. My hope, over the next few blogs is to unpack this a bit more, but here is a very brief summary:
If we want to have excellent, safe and financially sustainable health systems, we need four key ingredients, with the patient and their family at the heart/centre. The most important factor in providing safe and high quality care is a CULTURE OF JOY! I love this. I love that an institute based in Harvard, with research from across the world, is able to say this so clearly. If we have happy teams, we provide the best care. It’s simple! A culture of joy has three key elements: firstly the team needs to have a sense of camaraderie (we’re in this together and we love each other and take care of each other), secondly the team needs a sense of purpose and thirdly the members of the team need to feel trusted to do their jobs.
Alongside this culture of joy, there needs to be a SOCIAL MOVEMENT, both within the staff and in the wider society. A social movement relies on structures in which power is ceded and personal and corporate agency (responsibility and action) can flourish. There also needs to be a sense of CONTINUOUS LEARNING, in which all partake, every voice matters and no question is too stupid. In Toyota the staff make over 2.5 million suggestions each year! No wonder they are continually improving. And fourthly, there needs to be an agreed focus on QUALITY AND SAFETY, which entails several aspects.
All of this depends on a new kind of leadership that is first of all humble, able to cede power and deal with significant complexity and ‘not knowing’. When financial constraints are tight, or huge savings have to be made, it can be tempting to start rationing and cut services deeply. This may balance the books, temporarily, but it destroys every thing you are trying to build, demoralises staff, ruins your culture and breaks trust with those you are trying to serve. The challenge is to begin to hold our nerve in the midst of extreme pressure and do what we know is right, backed by the best evidence available to us – and this, believe it or not, actually makes us financially sustainable. I am going to really enjoy unpacking this more and revisiting my learning over the next few blogs, but the above should hopefully fuel some thinking in the mean time.
The IHI in Boston have proven that the joy of teams is the biggest single factor in patient satety and quality of care. Here is a 1 minute video highlighting the 5 key behaviours of CEOs, in healthcare organisations, that enable joy in their teams. If CEOs are not acting in these ways they are having a directly negative impact on patient safety and care and therefore might not be the right person for the job. #cultureofkindness #cultureofjoy #culturechange


































{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}