Yesterday, I tweeted that I think Dido Harding, the Chair of NHS Improvement and newly appointed head of the newly established National Institute for Public Protection (NIPP), which is to replace Public Health England (PHE), is a good leader. I say this, having met her and few times, through the NHS Assembly and her genuinely humble desire to listen and treat people with kindness. It caused quite an interesting discussion and there has been widespread criticism of her appointment.
Last week I did my yearly updates of the mandatory online training required in the NHS. Part of this included my ‘fraud awareness’ and this focuses, particularly on the Nolan principles – an ethical framework under which we are required to work. If these principles are not followed, people can quite rightly lose their jobs and even be sent to prison. The principles apply to all people who work in public life, not just the NHS and are as follows:
1. Selflessness
Holders of public office should take decisions solely in terms of the public interest.
2. Integrity
Holders of public office must avoid placing themselves under any obligation to people or organisations that might try inappropriately to influence them in their work. They should not act or take decisions in order to gain financial or other material benefits for themselves, their family, or their friends. They must declare and resolve any interests and relationships.
3. Objectivity
Holders of public office must act and take decisions impartially, fairly and on merit, using the best evidence and without discrimination or bias.
4. Accountability
Holders of public office are accountable for their decisions and actions to the public and must submit themselves to the scrutiny necessary to ensure this.
5. Openness
Holders of public office should act and take decisions in an open and transparent manner. Information should not be withheld from the public unless there are clear and lawful reasons for so doing.
6. Honesty
Holders of public office should be truthful.
7. Leadership
Holders of public office should exhibit these principles in their own behaviour. They should actively promote and robustly support the principles and be willing to challenge poor behaviour wherever it occurs.
from The Guardian
The decision to disband Public Health England, (which is recognised internationally as a world leader in the realm of Public Health) and the appointment of Dido Harding into her new role (even though I do really like and respect her) are not aligned with the Nolan principles and I believe therefore that the Secretary of State for Health and Social Care, Matt Hancock has some serious questions to answer, which are absolutely in the public interest. Each of those questions should be framed around the Nolan principles and are a part of the accountability required in such a momentous decision. It’s not that Dido Harding (who called for more integrity in NHS leadership) is necessarily the wrong person (although many feel that she is). It’s the way the appointment was made that makes everything so murky and this is a great shame.
Public Health England must not be used as a scapegoat in the forthcoming independent enquiry into the UK’s response to Covid-19. We must also better understand where and how its other vital functions will be performed. As Jeanelle de Gruchy, President of the Association of Directors of Public Health, has so eloquently argued, the NHS is not currently set up to do this work. There is the potential that the newly established Integrated Care Systems (ICS’) across England, which bring together public sector partners, including the NHS and local government could hold the responsibility, but this would need to be funded adequately and appropriately AND would require a legal framework, which is currently lacking. We simply cannot afford to lose the vital functions of prevention, child health and other huge programmes previously co-ordinated by PHE. With further financial issues ahead for local government, the idea that public health prevention will remain a priority, when we have already seen the roll back of this since 2010 is unrealistic. If this happens, rather than ‘levelling up’, the great promise of the Prime-minister, Boris Johnson, we will see a worsening health inequality gap and those in our poorest communities struggling even more.
We need urgent answers to urgent questions. But more than this, we need a government who are willing to act with integrity, openness and through the proper mechanisms of parliament. Announcing major changes to the functions of public sector organisations through the press and the refusal to follow good processes in redesign are seriously unwise and unfair. Trust in this government is waning and they could do a great deal more to rebuild that trust, if they care to do so. The loss of Public Health England matters, not only because it does such incredibly important work beyond public protection, but because of the manner in which it was disbanded and what this means about how government is functioning.
When Matt Hancock made his speech about his new NIPP yesterday, he finished his Q&A session by talking about the “Holy Trinity” of Academia, Government and the Private Sector. I see very little that is holy about this triad, especially if the Nolan principles are flouted. The Trinity I know is full of love and truth…..I wonder what the consequences of this clear ideology will have on the future of the NHS. I fear the answer is not in the public interest.
Last week Boris Johnson declared that we must do more to tackle Obesity, as the evidence has shown that it is a significant risk factor in increased mortality from Covid-19. Why it has taken this Coronavirus to wake the government up, I’m not quite sure, when we’ve known about the risk from obesity in terms of Type 2 Diabetes, Cancer, Musculoskeletal and Cardiovascular Disease for a very long time. However, the new strategy the government have released, is welcome, although it still puts too much emphasis on individual choice and fails to grasp some of the most important issues.
I’ve blogged on here previously about the complex nature of Obesity in our society. If we’re really going to tackle the issue of Obesity, we have to break the stigma of ‘fat-shaming’, undo the myth that it’s really just a simple matter of people ‘taking more responsibility, eating less and exercising more’ (see previous blog in which I draw on the phenomenal work of Prof Sandro Galea), understand the vast machine at work which is actually making us all more unhealthy and work out how we dismantle it and promote much greater wellbeing across society. There is no shame in being overweight. If everybody were slim and lithe, it would be very boring. However, being overweight (as indeed I am, currently) does lead us to have increased current and future health issues. With so many of us (67% of men and 60% of women) being over our ‘ideal’ BMI (body mass index) it’s causing us to live with more associated complexities and we do need to face this, however difficult it may be. We are told that Obesity is reported to cost £5.1 billion a year to the NHS…..But what does this mean to anyone except to induce more shame that their choices are costing the NHS and they should therefore change….it’s unhelpful and deeply demotivating.
This conversation cannot be about blame. It’s about examining the root causes. There are multiple levels of responsibility and complicity and so the answers are not simple, but are multifactoral. What I seek to do in this two-part Long-Read blog post is look at some of the deeper issues and where we might move forward into genuine solutions. This means owning up to mistakes and failures whilst finding a way forward together. What I do believe is that those who hold power and make decisions must take a greater share of this burden, rather than pushing it down onto the individual. On that basis, this blog-post will focus on all the other levels that can affect obesity and the following post will look at what individuals and communities can do/change in the light of this. I am not trying to give all the answers here. But I am trying to give a bit more provocation to the depth of debate and hope that we might take this conversation seriously.
Let us begin with National Government.
The National Government (particularly since 2010) has been woefully deficient in this entire situation. I say that, as the Marmot report highlights how inequality and health outcomes have worsened since that time. It has hidden behind the rhetoric of ‘free choice’, stubbornly believing that the ‘benevolent hand of the market’ will cause things to balance out. This libertarian approach is based on the notion that ‘the Nanny State’ is too interventionist and it is not the role of government to tell people how to live their lives. The government have turned a blind eye to corporate greed and irresponsibility, whilst blaming individuals for making poor choices, part of the ‘stigma machine‘ it has driven over the past decade to paint a picture of our poorest communities. Yet last year the food and drinks industry spent £143 million on advertising obesogenic products to the British public! As Shoshana Zuboff so powerfully demonstrates in her seminal work ‘Surveillance Capitalism‘, there is very little ‘free choice’ left in the world these days!
Johnson is perhaps waking up to just how fed up the nation is with ‘Austerity’, but many still believe that it was a ‘necessary evil‘ to dig us out of an economic black hole. It was a political choice. One that was unnecessary and one that has done great harm to the nation as a whole, but in particular to our most deprived communities, particularly when it comes to health outcomes. Tory Peers this week have shown just how inadequate ‘Universal Credit’ is, we continue to see a rise in the use of food banks (where healthy food choices are not altogether plentiful), fast rising admissions to hospital for children with malnutrition, falling life expectancy for women in our poorest communities, and significantly worsening obesity, again worse in areas of greater ‘deprivation’. All the while, the government pushed the responsibility for fixing this mess, primarily onto the individual but also onto local governments, through the realignment of public health in the coalition government reorganisation of the NHS. However, devastating cuts to these localities, meant a significant drop in public health spending. We’ve seen the loss of sure start, exercise programmes and healthy eating help (something the government is now wanting to replace, through a new scheme involving GPs).
It has taken Marcus Rashford to wake the government up to the effects of child hunger, though the summer holidays and further reports have shown just how inadequate the funding of schools is when it comes to tackling malnutrition. It’s a strange conundrum that obesity and malnutrition actually go together in our poorest communities. It’s all well and good telling individuals to get out and exercise, but with the loss of 21000 police officers, communities are now less safe, with many young children and teenagers unable to access local parks due to the associated increase in violent crime and gang crime, also linked with the loss of youth centres. Where are people supposed to exercise? In Morecambe Bay, a staggeringly high percentage of children in Barrow, have never visited the Lake District or even the beach! The same applies to Morecambe and Lancaster. Perhaps there is a solution, which I will come to later, but all this finger wagging, whilst cutting genuine accessibility due to poor transport networks, shows just how out of touch the government are with the effects of their own policies. Cutting theses services in the first place has made the health inequality gap widen.
On top of this, there has been almost no effective regulation of the sugar industry, which continues to pump more terrible calories into our food, without even telling us (and labelling hasn’t really helped, due to the ongoing power of advertising, BOGOFs and product placement). It’s important the government sorts out its own policies in this arena and its current proposals are not good enough, although they are at least a start in the right direction.
So, what does the government need to do?
1) It needs to ensure that Universal Credit actually works or consider a Universal Basic Income in its place. Poverty and Obesity are tightly aligned and current provision to tackle both is entirely inadequate. Until we see the demise of food banks, we will struggle to tackle the basics of health inequality. However, on current predictions, years of failed policies for our poorest communities will mean this will only increase as we enter a deep recession due to the double whammy of covid-19 and brexit.
2) It needs to stop the game of stigmatisation and the false blame of individuals. In her seminal work, ‘Stigma: The Machinery of Inequality’ (which I think is critical reading right now), Prof Imogen Tyler looks at how Stigma is weaponised by governments to inflict policies such as ‘Austerity’. These same mechanisms have been used when it comes to obesity and this kind of shaming must end.
3) It needs to get a grip of the Food (and in-particular Sugar) Industry. It needs to set tighter boundaries around advertising (good to see the beginnings of this in the new strategy), product placement and the content of sugar in products and stop hiding behind the nonsense of the nanny-state (again good to see a start on this by changing rules around advertising before the watershed). The Kingsfund (great work from David Buck) has clearly shown that people did not mind the intervention on smoking and would actually favour more government intervention in this field. The role of government, we are told, is to protect it’s people. There is so much more to do than the initial proposals being made.
4) The government needs to raise taxes on particular products, especially cakes and biscuits, to support nationwide behaviour change. Without this, it will be difficult to tackle ingrained behaviour. A century ago, chocolate was considered a luxury. We need to think of treats as exactly that and not a daily snack and price changes will cause this to happen better than almost anything else.
5) The government needs to put necessary protections in place for the Farming Industry and create legislation that moves us towards a more plant based diet, that is better for the human biome and tackles climate change, whilst also helping us to have healthier and more sustainable diets.
6) This may sound utterly controversial, but I believe may be a solution to help tackle both climate change and our health issues: they should consider rationing. We haven’t seen anything like this since WW2, but we’re in unprecedented times. If we are to ensure that everyone has enough and all people can eat well (therefore diminishing the need for food banks), whilst also helping us learn how to do so in a way that is not overindulgent, then this may be difficult but necessary medicine. How can we live in a world in which we throw away so much food, whilst millions go hungry? Would rationing help us to discipline ourselves and find a more sustainable and equitable future available to all? Heavy handed, I know, and probably laughable in some quarters, but maybe, during this pandemic, we should at least consider it – giving everyone a universal basic diet – I suppose it would be a bit like exploring a universal basic income – something which is gaining more support.
7) Central government must adequately fund local government, in particular public heath programmes and schools. The leader of Lancashire County Council has been clear with the Prime Minister, that the new allocation is well below what is needed for the task ahead. Does BJ have ears to listen? Do the government really understand the true power and nature of local governments and what they can achieve in partnership with the communities they serve? Look at what the Marmot Cities are beginning to achieve. Do we really want to stifle this? The healthy lifestyle programmes must be adequately funded and appropriately targeted towards areas with the greatest problems. They must also be designed in a way that encourages health rather than shaming ‘unhealth’.
8) The Government must take on the corporate giants. A few years ago, I started working with the Consumer Goods Forum (a network of manufacturers and retailers, with a combined global turnover over several trillion dollars) around how they might work more seriously in partnership with the NHS and PHE around the issue of obesity, diabetes and health inequality. I have to say that to date, although there is lots of willingness on paper, a combined effort is hampered by competition laws and the primary motivation of profit over all else. They could easily change product placement, especially at the tills; they could easily have been more on the front foot in helping us fight this crisis. Instead, they have tinkered around the edges, whilst raking in the profits. I hope now that they see just what obesity is causing in the complexities around Covid-19 that they might just finally take this a little bit more seriously and play their full part in changing this narrative. They say that they are simply meeting the demands of the public, and yet they are the ones who have spent colossal sums of money in advertising to convince us to buy products that do us harm and then pricing and placing them in a way that makes them utterly irresistible. I am therefore highly doubtful that they will change their behaviour unless forced to do so, which is why the government must be more interventional. Some of these companies don’t even pay their fair share of taxes, taking the profits whilst leaving the NHS to pick up the bill.
What Is the Role of Local Government?
I agree with Geoff Driver that the current promised funding for Local Government is terribly insufficient for the task ahead. However, with whatever package is finally agreed, there are certain things which I believe local councils must focus on. Firstly, they must take a collaborative approach WITH the communities they serve, building with and on community assets. Secondly, they must get a grip of local licensing of fast food restaurants and take-always – the current government proposals are unlikely to make much impact in inner city areas. Thirdly, they must invest in green and active transport, taking this opportunity to create many more cycle lanes and safe walking paths to ensure that they tackle both climate change and obesity in the same move. Finally, they must replace services they have cut and work in partnership with local NHS teams, especially primary care networks on the delivery of proven interventions.
The NHS
Some might think the NHS has quite a lot on its plate currently, but there is no doubt that it has an important role in tackling obesity. GPs and Practice Nurses have proven through great work around smoking, that they can make a significant difference as part of an overall strategy. However, given the complex nature of obesity, my recommendations would be as follows:
1) We need to talk much more about creating a trauma-informed approach. I would like to see the opening of ‘trauma-recovery centres’ in each of the regions of England and the other 3 nations. The reality is that obesity is massively linked to adversity experienced in childhood/adulthood and coping mechanisms associated with this. We need to stop asking people, ‘what is wrong with you?’ and be far more interested to find out ‘what happened to you?’ or ‘what is your story?’. Compassionate communities are those that recognise the complexity of our human lives and look at people with kind eyes, rather than judgement. It’s vital that this is more true than ever in the consultations room.
2) Leading on from this, we need to widen the use of ‘motivational interviewing’ and ‘coaching’ techniques, with help of the ‘patient activation measure’. We are using this with great effect in Morecambe Bay – it works with people so much more effectively than just telling them what to do. It enables people to feel empowered to make the changes they want to see in a way and a timescale that is realistic for them.
3) We must stop funding national programmes, which are ineffective (many of which are a total waste of time and money, in my opinion), and instead invest in helping PCNs listen to the actual needs of their community, through initiatives like the poverty truth commission, and then partner with those communities to bring about real, lasting, relational and effective change. If you compare what local PCN programmes are achieving around Type 2 diabetes reversal compared to the National Diabetes Prevention Programme (NDPP), which the government have given a further committment to rolling out, you would scrap the NDPP and invest far more in local communities, which are much cheaper and significantly more effective. Local relationships and expertise trump nationally driven campaigns every day of the week.
4) We have to look at the GP model and provision of care in our economically poorest communities. It has to be more attractive and we need to be braver at putting funding where it is needed the most. We won’t break down health inequalities, if we don’t get more clinicians working in and with those who are struggling the most.
5) We need to encourage better partnerships between GP practices and local schools in working towards a healthier place-based curriculum. We’re very blessed in Morecambe Bay to be working on this with the fabulous Eden Project North, but not everyone has this on their doorstep…..so what is possible in each locality?
6) Hospitals need to be doing much more with the money they are already given in making sure that ‘pre-hab’, prior to surgery is far more effective. I am aware of hospital trusts in which high percentages of patients are having routine knee and hip replacements, and routine abdominal surgery (like hernia repairs and cholecystectomies – gallbladder removals) with very high BMIs. Not only is this actually unsafe, it leads to much longer stays in hospital afterwards, driving up the overall cost the procedures. If hospital teams were dedicated to helping people achieve optimal weight before surgery, the number of people actually needing that surgery would dramatically reduce. We are currently implementing such a model in Morecambe Bay, thanks to a great partnership between GPs, Surgeons, Managers and Commissioners.
7) We need to see a faster integration of PCN teams to include Health Visitors and possibly, community midwives. The first 1000 days of a child’s life are vital at determining the course of the the rest of it’s long term wellbeing. Working with the ‘maternal commons’ and changing the tide for the future generations is vital. Things like Breast Feeding (which can reduce obesity by 25%!) and healthy snacks need to become the norm in all our communities.
Employers Have a Key Role!
The work place environment is often incredibly unhealthy. However, we have learned together, through this current pandemic, that it really is possible for us to work differently. Greater workplace flexibility to encourage exercise breaks, healthy eating in the work place and active travel should now become routine parts of the day. It makes total economic sense. A happy and healthy workforce are more likely to stick with a company and have less time off sick. It’s absolutely vital that we end ‘in-work poverty’ by seeing a true living wage across the UK. It’s one of the reasons I am so passionate about seeing the NHS as an anchor institution in each area through the UK, partnering with other organisations to set the standard of good employment. The new NHS people plan sets us firmly in the right direction.
National Parks/The National Trust/Areas of Outstanding Natural Beauty
I would love to see an agreement between the department for education, local governments and these national treasures to become much more widely available to children from our poorest communities. These places are primarily now the playgrounds of the middle-class only, but this is unacceptable. How can we ensure that all our children can enjoy the delights of the counties across the UK, and not just the privileged few? How can we make it more affordable for communities to get to these places, pay the entrance fee (where warranted) or believe that they are really for them? The National Trust was set up for the poor…..can it rediscover what it exists for?
Schools
Schools are underfunded and teachers are underpaid – let me just put that out there, before making any recommendations. The amount that teachers are now having to deal with in their classrooms around hunger alone, is beyond unacceptable. Children in our poorest communities are eating highly processed and insufficiently nutritious food, leaving them both overweight and malnourished simultaneously. We desperately need to build a curriculum around food security and physical and mental wellbeing. The focus is currently wrong and we are punishing children who are too hungry to learn. We must also think creatively about the timetabling of Physical Education, especially for our young women. The link between maternal obesity and the child’s future poor cardiovascular health is staggering. I recently did some listening with some teenage young women, who told me plainly about the jeering they continually get from boys when in their PE outfits, the horrors of having PE in the first period and then feeling red and hot and sweaty all day and therefore the high numbers of ‘drop-outs’ from PE lessons. Exercise is such a vital part of life, helps us focus on our work and have better mental health outcomes. Given the crisis we are facing, both around mental and physical wellbeing in our schools, is it time to radically rethink the school uniform, the PE ‘offer’ and how we might move towards a more inclusive and less ‘macho’ PE culture? Alongside this, we need to look at the quality of school meals – surely we can do better?!
Conclusion
The current narrative around obesity is full of stigmatisation and is grossly oversimplified. I hope that this blog has highlighted some of the complexity involved and therefore why we should approach the discussion with more humility and compassion. Of course individual people and communities have a role to play in the choices they make and the behaviours they adopt (and in my next blog, I will give more thought and focus to this), but for too long, we have made that the focus and forgotten about the enormous environmental factors which have caused the situation we find ourselves in. We will have to see just how serious the government is about really addressing the health inequalities in our nation. Obesity is a good ‘test-case’ and will mean a major sea change in policy and implementation at every level of society. I hope this blog goes some way to stimulating even more debate about how we break the stigma of obesity and find solutions which genuinely change the outcomes for Marmot 2030!
I recently wrote a blog about reimagining health and care in this apocalyptic moment. In this post, I want to put a bit more flesh on the bones of what that might actually look in the context of the NHS, here in the UK and particularly, England.
Let me just make a few statements about where I’m at when thinking about future health and care:
I believe in a publicly funded and provided national health and care service, paid for through fair taxation.
I believe that health and care should be available to all people, equally, regardless of ability to pay.
I believe in locally led health and care systems, embedded in local communities.
I believe prevention is better than cure and we need to get up stream and stop people falling in the river in the first place.
I believe creating great working cultures enables teams to flourish and brings out the best in people. I know right now that our health and care workforce is feeling burnt out and overwhelmed. We can’t keep working under the huge burdens of constantly changing goal posts, key performance indicators and heavily mandated targets. The wellbeing of those who work in this sector has been overlooked for too long and the stress levels caused by the sheer pace and volume of work are not acceptable.
I believe there is systemic and ingrained racism in our communities and within the NHS and even though I consider myself to be ‘woke’ about this, as a privileged, white, male, there is still so much work for me and us to do, both internally and externally in order to break the curse of white supremacy. It is simply not enough to say ‘black lives matter’ – our words are cheap unless we do not confront internalised narratives and change society together, from the inside-out through truth and action.
I believe our economic system is no longer fit for the 21st century and am so grateful for the reimagining of what economics is for.
I believe the role of government needs to radically change to be much more empowering of local communities, with appropriate frameworks to support this. We are seeing the mess of centralised control, with unchecked and wasteful investment in the private sector, rather than local community empowerment in this current Covid-19 pandemic.
I believe communities are able to self-organise phenomenally well, as we have seen throughout this pandemic and should be supported to do so more through a much more participatory and relational politics.
I believe that any health and care service should promote overall wellbeing by paying extra special attention to:
instating women fully and equally
prioritising children
advocating for the poor and breaking down health inequalities especially through challenging stigma (Very grateful to Imogen Tyler for her great work on this)
welcoming ‘strangers’ (by this I particularly mean the way we treat staff from overseas and how we care for refugees and asylum seekers)
reintegrating humanity with the environment (e.g. by getting back to basics of nutrition and sustainable food)
restoring justice to prisoners (metaphorical and real)
healing the sick – through both slow and fast medicine
ensure the honouring the elderly In how they are cared for
So……(!)……How do we take the best thinking around health and care systems and make it real and practicable in the NHS and Care System? Firstly, I suggest that we need to take the hierarchical, pyramidal system and simply flip it upside down. Let’s begin at the local level, as the foundations stones of a reimagined health and care system and build from there. With this we need to take seriously what Simon Parker is calling for in a rethink of what government exists for.
Within the health and care system though, we don’t another fresh reorganisation. We have some good things we can play around with. We just need to stretch our thinking a bit more and permission some creative, entrepreneurial experiments and we can see something really exciting emerge. Primary Care Networks are a good basic building block, which take the best of clinical leadership, and when done properly, combine it with local communities to build local health and wellbeing. They cause General Practice to work together more collaboratively, use the best of available data to map the issues a population are facing and have the flexibility to begin working differently. They are not perfect, and in my opinion, need some adaptation, if they are going to enable the tackling of health inequalities, social injustice and true community empowerment.
Firstly, they need more time. The phrase ‘at pace and scale’, used all too often in various management discussions In the health sector, is the antithesis of what the NHS needs right now. PCNs need time to build stronger relationships with their local communities, really listen to what their community are experiencing and build local solutions WITH their communities through co-design and co-creation. The constant onslaught of new targets, new measurement tools, new initiatives, all to be delivered by, well, yesterday, are completely counterproductive to the transition and revolution that community medicine needs to make. The current work load in General Practice is unsafe and unsustainable and is a byproduct of the consumerist attitude we have taken towards healthcare as a commodity. PCNs need time and will fail otherwise! This must be created for them.
Secondly, PCNs need to look at alternative and more sustainable models for the future. Currently, PCNs are very much built around General Practice at the core, and this makes alot of sense in many ways. However, here in Morecambe Bay, we have a building block called ‘Integrated Care Communities’ (ICCs), which pre-date PCNs by some five years. I believe we need to see a melding of the best bits of both, with a much wider and more integrated team within and around the PCN model. The traditional GP partnership model, though highly successful and desirable in so many ways, continues to build a model with the GP, primarily as the leader. I am a GP Partner myself – there are some huge benefits to such a model, especially often through great altruism and genuine community care. One of the difficulties facing primary care, as it stands though, is that few ‘future GPs’ want to become partners, preferring a ‘salaried’ approach and the issues facing primary care may, perhaps require a different kind of (and perhaps more socially just) economic model. I suggest that PCNs may want to explore the highly effective and entrepreneurial model of Social Cooperatives. Such models have proved highly successful in places like The Netherlands and New Zealand, provide greater sustainability, better collaborative working and more exciting opportunities. Drawing on the work of the economists, Spencer Thompson, Kate Raworth, Mariana Mazzucato, Katherine Trebeck (and others) I can see that a social co-operative model of PCNs, given trust and freedom to experiment, by either government or commissioners, could really remodel health and care at a local level, around genuine community need, as set out by Hilary Cottam in Radical Help. We could see the creation of locally led (and owned) community health and care services (perhaps even including care homes, who are still very poorly treated as we have seen through this crisis), creating healthy communities from pre-conception to death through asset based community development and participatory, democratic processes. A social cooperative model allows all people working together in a geography to be part of the same ‘system‘, rather than the current clumsiness of multiple ‘sovereign organisations’ tripping over each other, whilst creating similar community roles, bespoke to each employer’s whim. However, a cooperative model may not work for all organisations, like the police and fire-service (I’m happy to be convinced otherwise) and so building relationships, sharing milk and working having regular check-ins and multidisciplinary team meetings will continue to be important.
The possibilities at the local level are endless. PCNs would be able to prioritise a much more proactive, preventative model of health and care, employing smaller but more relational and therefore more effective and sustainable teams, embedded in local communities. They would form fantastic partnerships with local schools, co-designing a curriculum that creates positive mental and physical health, connecting young people more into their community and environment whilst being trauma-informed and compassionate in their leadership. Midwives, health visitors, social workers, community Paediatricians and mental health practitioners could form part of the core team and all work from the same geographical space with IT systems that actually talk to each other. Community care of the elderly would be more joined up, with care of the elderly physicians leading their own care of nursing home patients, supported by specialist nurse practitioners, along with, of course the incredible 3rd sector. It might be that some consultants, e.g. Rheumatologists, Dermatologists and Psychiatrists could belong to a cohort of PCNs, even employed by them, and therefore create a greater sense of belonging to a particular set of communities and they would also be able to work with communities more proactively through workshops, group consultations and education settings. Teams could flex and grow to suit the needs of a community, with the economic model set up to enable rather than constrain the flourishing of such initiatives. The social cooperatives could also form community land trusts which could begin to tackle various wider social determinants of poor health, including issues like housing, homelessness and access to green spaces. These cooperatives could ensure a living wage and persuade local businesses to get more involved in the area of health and wellbeing and even invest in the kind of initiatives that would create work in the green sector for local people. Why shouldn’t local health communities be involved in social change, when these issues affect the health of their communities so vastly?
I see local leadership teams (what we call Integrated Care Partnerships or ICPs), made up of PCN Directors, Local Government Officials, CVFS CEOs, The Police, Fire Service and Hospital Chiefs continuing to take the role of looking at a wider Population, made up of a group of PCNs and support them in tackling health inequalities, taking a servant leadership approach to empower them to succeed as much as possible. Primarily this group would be about permissioning, enabling, encouraging, holding space for learning and development, holding true to values and using data to facilitate excellence in practice. Relationships and trust will be the core ‘operating framework’ to enable PCNs to fully flourish.
The Integrated Care System (ICS) Leaders then need to take a similar approach with each ICP in their domain, giving as much power away as possible and taking a collaborative approach across a wider geography to learn from each other and encourage best practice and through the sharing of stories and success. It’s this kind of nurturing and facilitative leadership that will enable each ICP and PCN to flourish. Hospitals will naturally become more focused on acute care, and areas, like Oncolgy, as consultants become more aligned to the PCNs with which they primarily work (obviously this does not apply to all specialities, which is why an ICS can take more of an overall look at the hospital requirements for the population it serves). The role of the national NHS England and NHS Improvement teams then becomes the servant of all, the enabler and the holder of core values. Rather than a central command and control structure, it gives itself to a love-poured out model, creating cultures of joy right through the health and care system. Yes, it sets some priorities, but does so by listening to what communities around the nation are saying. So right now that would include asking PCNs to prioritise tackling systemic and ingrained racism, health inequalities and childhood trauma, in collaboration with their communities. They will take the best of international experience and learning, share that widely and reimagine the NHS as global trend-setter for how we create deep peace and wellbeing in our communities, enabling us to become good ancestors of the future. A radical, revolutionary but entirely practical refocusing of the NHS and Care System from the bottom-up is entirely possible. There is almost no remodelling needed, simply a change in focus and culture. It requires PCNs and the communities they serve to get on an do it together, disregarding that which prevents them. If they do this, they will find that everything they need will follow them and their light will shine brightly.
There is a ‘kairos moment’ available to us to reimagine how we think about health and care, here in the UK and indeed globally. It’s true that COVID-19 is going to continue to take our attention and shape our health and care services in a particular way for many months ahead. But some have been talking about COVID-19 as an apocalyptic event. The word apocalypse literally means “to lift the veil” i.e. it causes us to see what is behind the facades. Therefore, if we are living through some kind of apocalypse, let us see with new and clear eyes what it is showing to us. If the facades are down – what is it that we are now seeing in plain sight, which may have been previously hidden from us and what are we going to change as a result? COVID-19 is exposing for us, yet again, what Michael Marmot has been telling us for years, that poor health affects our economically poorer communities and poverty kills. We cannot ignore the greater impact felt by those of our BAME citizens and what this speaks to us. We see theburnout of NHS and Social Care Staff highlighted by Prof Michael West, even more clearly, just how valued they are by the publicand the unsustainable nature of their workload, caused by long hours, high demands and under resource. So what kind of health and care service does the future need?
In the UK, we have a health system that responds brilliantly to crisis (in the most part). We’re by no means perfect, but we do acute care really rather well. But overall, although the WHO rates our health system as one of the best in the world, our current system approach is not tackling health inequality, it is not coping with the huge mental health crisis and it is floundering with the cuts to local government and our ability to work in an upstream preventative way. Meanwhile, our over-busy, over-hurried workforce don’t have the time to really care for themselves (thus huge levels of burnout and low staff morale) or bring genuine, lasting therapeutic healing to our communities. I cannot tell you how many NHS and Social care professionals I see in my clinic at the point of despair. I know of whole social care teams who have cried under their desks and vomited into the bins in their offices because of the untold pressure they feel under to manage hugely complex and unsafe portfolios. Now is the moment when we have to grasp the nettle and accept that we can’t go back there. I don’t want to. My friends and colleagues don’t want to and truly, we simply can’t afford to.
Our health and care system tends to focus on short-term (political) gains and quick, demonstrable change, rather than the bigger ticket items around genuine population health. Sometimes we just change things for the sake of changing things but without a focus on what it is that we really want to see change. It’s exhausting. We can quickly build several new Nightingale Hospitals (which thankfully we haven’t needed), but we haven’t been able to ensure wide-scale testing, contact tracing and appropriate isolation. We can easily promise to build 40 new hospitals and feel excited by this prospect, but we have seen a decreasing life expectancy in women from our economically most deprived communities and a worsening gap in life expectancy. We need a health and care system which creates health and wellbeing in our communities, while maintaining the ability to respond to crises.
My friend, Hilary Cottam has written in her book ‘Radical Help’ abut the reimagining of the Welfare State for the 21st Century, with some superb examples of what can be made possible, especially within the realm of Social Care, for all age groups. Where this was applied most widely in Wigan, under the beautifully humble, kind, collaborative and inclusive leadership of then Chief Executive, Prof Donna Hall, the results were and continue to be staggering. One of the devastating parts of Hilary’s book is to read her chapter on experiments in the NHS. They were hugely successful, saved money and delivered better care, but when push came to shove, commissioners couldn’t extract funding from where it was to invest in the ‘brave new world’. It would be possible to conclude that the kind of transformation we need to see in the NHS is not currently possible – partly related to culture and partly because of centrally driven targets, which make brave financial choices hard to make with associated adverse political backlash. But I remain optimistic!As we look towards a desperately needed, more integrated health and care system, I believe if we applied Hilary’s 6 core principles with some audacity, we might see some amazing things occur in our communities.
For me, the change must begin from the inside – if we do not get our culture right (and we still have some significant issues around bullying, discrimination, staff well-being and poor citizen care) then it won’t matter what we do structurally or how we reorganise ourselves. If you haven’t seen my TEDx talk about how we create the kind of culture that allows us to do this, then you might find it helpful to watch it here.
Hilary’s six steps give us a really good platform from which to reimagine and build a health and care system fit for the future that is calling us:
Grow the Good Life!
We know that COVID has primarily affected our more economically poor areas with a significantly higher mortality rate. This is not news, but perhaps we see it more starkly in the light of this current pandemic. Michael Marmot has been telling us this for decades but his recent report (link above) highlights for us the decline in health outcomes and worsening health inequalities, since 2010. Firstly, we must recognise that the good life is not supposed to be only for the rich and nor does money necessarily lead to a ‘good life’. The good life is for everyone, everywhere. Secondly, we must accept that the good life is something which is not shaped by the powerful on behalf of communities. It is grown, fostered and tended by communities themselves, who own the mandate that ‘nothing about us without us, is for us’. Thirdly, we must therefore stop taking a reactionary approach to health and care and create wellness in and with our communities, determined to break down age-old health inequalities, tackle poverty, poor housing and climate change. We must accept that we cannot fix the problem and there will be no real health for our communities unless we cultivate the space for the good life to grow. A good place to start would be with a Universal Basic Income. It also means working across the public and business sectors to think about how we can be good employers and create the kind of jobs that the world really needs in the 21st Century – I’m excited to see that conversation alive and well, here in Morecambe Bay, particularly in Barrow-in-Furness and in Lancaster and Morecambe. It means ensuring that everyone has a home and access to good and clean transport. The good life must include a good start in life (and reverse the tide of childhood trauma), good opportunities to learn and develop (within a reset learning/education sector), good community, good work, good ageing and a good death. The good life enables us to be a good citizen, locally and globally and therefore the good life leads to a regenerated ecology. The good life must also include a good safety net if life falls apart or hard times come and really good care for those who live with the reality of chronic ill (physical and/or mental) health. The good life ensures that the elderly are honoured and cared for. It cannot be stated strongly enough that if we do not grow the good life then we will continue with the same old issues and the ongoing inequalities for generations to come. Health is primarily an economic issue and so all economic policies and choices show us who and what we value. Where do we need to shift our priorities and our resources in order to grow the good life together? Let us see beneath and behind the facades exposed in this moment and be determined that together we must co-create a much kinder and more compassionate society. There are so many economists (e.g. Mariana Mazzucato on how we create value, Kate Raworth on an Economics worthy of the 21st Century,Katherine Trebeck on why we need a Wellbeing Economy) doing great work on this. Why aren’t we listening to them more? Perhaps we are. 80% of people in the UK now want health and wellbeing to be prioritised over Economic Growth!
Develop Capability
Cormac Russell, the fantastic advocate of ABCD and all round champion of community power recently said this:
“The truth is, ‘the needed’ need ‘the needy’ more than ‘the needy’ need ‘the needed’. Society perpetuates the opposite story; because there’s an entire segment of the economy tied up in commodifying human needs. It’s a soft form of colonisation. That’s what needs to change.”
Perhaps, if the NHS and/or Social Care were a personality type on the Enneagram, it would be Type 2, or in other words it has a need to be needed. Perhaps we are the ones afraid of removing the ‘medical model’ and trusting people and communities to figure it out themselves – time, as we often say is a great diagnostic tool and a great healer. Many little niggles and issues often sort themselves out on their own, or with a good listening ear, or a change in diet, or some other remedy. What if, instead of trying to manage unmanageable need (at least a portion of which we have created ourselves by the very way we have designed our systems and through the narratives we tell our communities), we develop real capability in and with our communities? We have been interested in the world of General Practice how many people haven’t been in contact with us during COVID-19. I think the reasons for this in some ways are obvious (people were told to stay at home and so they did just that, and they wanted to protect the NHS, so they didn’t want to bother us) but in others are perhaps more complex and not necessarily altogether good – meaning we are seeing far few people with potential symptoms of more worrying conditions, like suspected cancers of various sorts. How do we design a system that starts with the good life, enhances community well-being, enables better collaborative care within and from communities themselves, whilst being able to respond to real need?
Surely people who live with various health conditions, or who have social needs should be in the driving seat when it comes to understanding their own condition or situation, recognising what their options are and deciding how to manage the care they receive. We must take a less paternalist approach to health and care and focus much more on coaching, empowerment and collaboration. Services will only really work for the people who need them, when they are co-designed by them. We will find this is much more cost effective, wholly more satisfying for all involved and will create a virtuous circle in creating the good life. Social prescribing goes some of the way, but is still way too prescriptive. This is about taking a step back and building understanding and creating more capability to live well in our communities, by focusing on a building on the strengths which are already there. We will only do this if we dare enough to really listen, putting aside what we presume we know and start a new conversation with our communities about what we really need together. We can do this in multiple ways, making the best use of available technology.
Above All Relationships
I believe relationship is pretty much at the heart of everything meaningful. If we’re really going to create the kind of health and care system that is fit for the 21st century, it’s not that we need to be less professional, it’s that we need to become more relational, step out from behind our lanyards and turn up as human beings first and foremost. When we really listen to the communities we serve we discover what a wasteful disservice we provide to the public in our current transactional approach. Yes we tick the boxes that keep our paymasters happy and fulfil our stringent KPIs, but in doing so, we spectacularly miss the point. Hilary’s chapter on the power of relationships in family social care is particularly poignant on this issue. If we plot the kind of interventions we make with perhaps the most troubled members of our community from a social care, mental health, policing and physical health perspective; we find that we make hundreds of contacts, spend an inordinate amount of money and see very little change for the fruit of our labour. What a waste! But when we ask these families what they really need, what their hopes and dreams are and how we might work with them to make this possible – yes there are bumps along the way, but we find with smaller and less expensive teams, we can achieve far more, because relationships are consistent, build trust and create the environment needed for real support and transformation. Why would we persist with a model that is outdated and doesn’t work?! Why are we afraid to work differently? We have to stop doing to and be together with. I believe Primary Care Networks create the kind of framework that begin to make this more possible. I think that if we see health visitors, school nurses, physios, SLTs, OTs, mental health teams and social workers integrated into these teams, we will see far more joined-up, cost-effective and relational care in and with our communities. In some ways, it doesn’t even matter who the ’employer’ is as long as we allow teams to work in a really inter-dependent way.
Connect Multiple Forms of Resource
If we keep working in silos and continue to measure outcomes by single organisations, we will continue to fail the public, waste money and exhaust our staff. However, if we can agree on good outcomes in collaboration with the public we serve, join up our local budgets, share our public resources and empower our teams to work in a truly integrated and collaborative culture (as has been happening through this pandemic), then we can begin to make a real difference where it is needed and see lasting change in our communities. In Morecambe Bay, our integrated teams are working in this way but there is more for us to do and further for us to go. One of the things I have particularly loved about the Wigan vision is the core 3 things they ask for from all their staff – Be Positive (take pride in all that you do), Be Accountable (be responsible for making things better), Be Courageous (be open to doing things differently). Three simple principles have enabled a fresh mindset and a new way of working which is clearly seen across their public sector teams and in the community at large. If we don’t learn to co-commission in partnership with our communities and across our organisations, we will not shift the resources from where they are to where they need to be. It’s definitely easier in the context of a unitary authority, but not impossible, if the relationships are good, in other contexts also. However, as Donna Hall argues, commissioning often gets in the way and is a blocker, rather than an enabler of resources getting into the right places because of the rule books involved. Her experience and track-record are well worth listening to, uncomfortable though they may be for those of us who work in commissioning organisations. Scotland doesn’t commission health and care in the way England does – are there lessons to learn? I don’t know the answer, but it is worth a conversation. What we do need for sure is thinner walls, blurred boundaries, greater humility, genuine trust, greater collaboration, real honesty, mutual accountability and true integration between ‘sovereign’ public organisations and the overstretched and over-burdened community-voluntary sector and yes, the private sector (….this talk by economist Mariana Mazzucato on how innovation happens is really worth thinking about). If we allow ourselves to do this, we will be on the way to a welfare system that is much more sustainable and practical.
Create Possibility
Go on! Try it! It’s OK to fail! We’ve got your back! If it seems like a good idea, give it a try! These are things we need to say and hear much more in the world of health and care. Of course we need to be guided by evidence, but there are so many things we do every day, because ‘that’s the way we do it’, often governed by a culture of fear. What might be made possible if we garnered a real sense of innovation, creativity, bravery and experimentation instead? But this must not just be limited to our teams. What are the possibilities within our communities. How do they see things. What hopes do they carry? What opportunities have they noticed for more kindness, better integration, smarter working and improved services? Are the services we provide really meeting the need? If not, what is possible instead? There is an ancient proverb that says: “Hope deferred makes the heart sick, but hope coming is a tree of life…” I wonder how much of the current ‘sickness’ we see in our communities is because people have lost a sense of hope that they can be part of any meaningful change. Just imagine how much life, health and well-being would be released into local streets and neighbourhoods, simply by including people in the participatory experience of dreaming about and actually building a better future that is more socially just and environmentally sustainable. In Wigan – this looked like The Wigan Deal. We need to take a similar approach everywhere – it’s not about replicating it – it’s great to learn from best practice and implement it more widely. But it’s also important that we start from a place of deep listening and creating hope and possibility. Change happens best when it comes from local, grass roots communities, who love and take a greater sense of responsibilities for the areas which they know and love. If this is going to happen, we have to embrace the notion of New Power!
Open: Take Care of Everyone
Our target driven culture is the enemy of creating really good health and care in our communities. Small minded, measurement-obsessed, top-down, KPI-driven, bureaucratic micro-management is strangling the life out of our public services and preventing us from reimagining a welfare state, especially concerning social care that we so desperately need. We can no longer tolerate the staggering inequalities experienced by our poorest communities and therefore we can no longer contemplate continuing to accept the silo’d and misaligned (under) funding of local government, social care and the NHS. If we are going to have a society that is caring to everyone, no matter of their age, gender, genome or race, then we must be determined to build a system on the values we hold dear of love, hope, inclusivity, joy and kindness. There is no way that we can do this from within the system alone. But the future is calling us to explore new paths together and build a system with much more flexibility and adaptability. This is not outside of our gift, nor beyond our reach. We cannot do it alone. But if we let go of any fear of localism and wide participation, then together, with our communities, in the places where we live, we can create a society that truly cares.
The world has changed. We cannot go back to where we were, nor continue to head in the same direction we were set upon before this crisis. But that is easier said than done and will be impossible if we do not embrace the grief of what we are journeying through together. There has been and continues to be painful loss. We have lost dear friends, family members, neighbours and colleagues. We have lost jobs, income, holidays and social gatherings. We have missed births and birthdays, key social events, final goodbyes and funerals. We are bereaved of whole ways of behaving – our ways of life, everything we’ve known has been entirely interrupted.
For me, as a type 7 on the Enneagram, it’s all too easy to engage in the future, to think about the ‘what next?’, to avoid the pain of the here and now, by letting my imagination run wild of what the world might be like instead. But we cannot and must not miss the vital part of our current journey, which is to recognise, embrace and partake in the grieving process. Grief is not comfortable, it is not easy, it is not enjoyable – in fact it is both tumultuous and painful…..but it is good. Refusing to enter into it, or trying to suppress it, will only lead to a deepening of the trauma and a delay of this inevitable experience.
The thing about grief is that it is unpredictable and what makes it even more so in this current experience is that it is both personal and corporate. However, the cycle of grief is well known and although each of us will go through the cycle differently, it’s worth recognising where in the cycle we might be, both as individuals and as a wider community/society.
This is the classic ‘grief cycle’ (I’ve borrowed the graphic from psychcentral.com) and it demonstrates well how the experience of grief is neither straightforward nor easy. However, psychologists agree that each of us will pass through each of these phases, no matter how briefly – though we can remain stuck in some areas for quite some time.
The isolation of this time has been the starting place for most of us. For some that was coupled with an acceptance that we are where we are, but for others there was a denial that this could be real and a refusal to engage with the idea of social distancing (although with police enforcement, this quickly began to change!).
The anger phase is clearly present for many at the moment, and understandably so. Anger is not wrong, it’s how we respond to it that becomes the issue. Sadly, in many households we’re seeing a rise in Domestic Violence , particularly towards women and children and this is something we need to take really seriously. Learning to control our anger and find a positive outlet for it is absolutely key. There are all kinds of online resources to help with this, but the deep cuts to social services and policing over recent years have made it difficult to work with families in a more proactive way. The Violence Reduction Unit in Lancashire, led by Detective Chief Superintendent Sue Clarke, who is a brilliant leader, have done some incredible work in this area over the past couple of years, which is well worth learning from. The approach is much more productive than traditional methods of dealing with this issue and involves being with families more proactively to bring restoration and redemption into broken situations.
These are all important questions that require an answer. Anger can be used to facilitate the right kind of conversations to bring challenge to the status quo and demand that it never leads us here again. The outcomes we are seeing were not inevitable – so what will we learn? What will be different? How will we change? If people in positions of power are willing to own up to mistakes, are we willing to forgive? I hope so…..how do we rebuild society otherwise? We must be able to learn and change our ways. It’s at the heart of what it means to love. But we must also recognise that some of this anger is simply part of the grief cycle and there may be no answers. We’re angry in part, because we are grieving. Sometimes our anger brings challenge and change, but sometimes we yell into the night and are met with silence.
Depression in grief can become clinical depression, but the word, in the context of grief, more describes a sense of deep sadness, loss, numbness, apathy and is often accompanied by tears. We must not try and keep a stiff upper lip, or push this away. Some of us will feel this more acutely than others, depending on our personality type, but this is a vitally important part of the process. This deep sadness can catch us unawares. It can come almost out of nowhere and we can find ourselves having a good cry in the bath or struggling to find the motivation to get out of bed of a morning. Talking about these feelings is absolutely vital, and it’s important that those of us who listen, ensure that the person experiencing these emotions feels heard. They don’t need fixing. They need validating. They need to know it’s OK to feel like this. We can’t just wish it away or get back on with things. There is a certain wallowing in this place that is extremely healthy and right. It’s true, we don’t want to get stuck here, and by putting some positive measures in place, like exercising, eating well, mindfulness and keeping a positive sense of routine, we can avoid becoming more mentally unwell. However, we must not try and rush through this phase or refuse to embrace the pain of it. But this can become a very dark experience and some people will wonder if life is even worth living. We can find ourselves asking searching questions: Can we really go on without our loved one? Will we ever get through the brokenness of this current situation, when we have lost so much? If this becomes overwhelming or there are serious thoughts of not wanting to carry on with life, this is where therapeutic interventions or medical treatment in the form of medication can be really important and literally life-saving.
At a corporate level, we share a sadness that 20000 people in the UK and 200000 people globally have lost their lives so far, due to COVID-19 – and that is just the recorded deaths. We will potentially feel lost that a whole way of being together is no longer possible, nor perhaps, desired. The artists will help us the most here. Songwriters, painters, choreographers and playwrights. Are we mature enough to embrace the songs and dances of lament? DO we know how to do this?
Bargaining is about us trying to begin to formulate some meaning or sense of what has happened/is happening. We might find that we want to talk about our experiences more, tell our stories, reach out to others and explore some of the ‘why’ questions we’re wrestling with. We might find we start ‘big conversations’ with God or ‘the universe’ – some thing like – ‘if you help me get my job back, then I’ll live a good life from now on’ or we might find we’re dealing with several regrets in our interactions or relationship with the person we have lost.
Acceptance is about realising that we are where we are and we cannot change a thing. It allows us to breathe deeply into the reality of the horrors we have walked through and begin to face into the future. Some people think of the grief cycle as more like a river with the grief cycle being a whirlpool that we get stuck in for a while. We go round and round, but eventually we come out the other side. On a personal level, perhaps, before we entered the whirlpool, we had a dearly loved one in our boat with us and we entered this whirlpool once that person became sick or was no longer in the boat with us, because they had died. The whirlpool can feel overwhelmingly difficult, with the stages above. We come out of the whirlpool with an acceptance that this dearly loved person is no longer in the boat with us….but there are other boats that we travel alongside, and perhaps there are others who still remain in our boat. We must now learn to live in this boat, without the person who was with us before but knowing we can face the future with our other companions. At a corporate level, this is about us sense making that the future cannot be like the past. Things have fundamentally changed. We cannot go back to how things were and so together we can build an altogether fairer and kinder future for our global population and the planet we inhabit together. This becomes what some refer to as the 6th stage of grief – ‘Meaning’. We begin to make sense of what we have journeyed through and use it to transform our experience of the world and how we want to live in it. My next blog will explore some of the meaning we may find the other side of COVID-19.
Whatever your experience of grief at this time, embrace it and talk about it, but don’t try and hurry it away. Good grief is a part of life and enables to process our loss, feel our pain, heal our wounds, accept our scars and find a new future. The ‘Good Grief’ movement is something I would really recommend exploring, especially if you are struggling to process your own grief. There is also lots of mental health support available through your local GP or online via nhs.uk. Grieving allows us not only to engage with the pain we are going through, but allows us to let go, so that we can reset and rediscover a way forward together. It’s impossible to walk through it alone, which is why as the city of Liverpool reminds us in the amazing song, sung at Anfield, friendship is everything.
Kate Raworth’s work on the Doughnut Economy over the last few years has been nothing short of extraordinary. She has torn up the economic text books of the last 150 years and asked some much better and kinder questions about the future we need. It is so exciting to read that in collaboration with Janine Benyus, using biomimicry, the model is now being implemented in the City of Amsterdam. It opens up a world of possibility for a reimagined future, in which our world becomes regenerated for both people and the planet itself.
Kate’s book and then her blog deserve serious attention and, in my opinion, a Nobel Prize! There is no way in this short blog that I can even begin to explore the exponential potential of the work, but I do want to highlight some of the key issues. So many people are saying that we simply can’t go back to how things were prior to Covid-19. If we’re serious about that statement then we need to begin thinking about how we will experiment with alternative models and ways of being together that will be good for the future of the environment and create a much more socially just framework for the global family of humanity. I love this model that Kate offers in thinking about what is important for a place – it contains four key aspects. Local/Global – Social/Ecological.
We can apply this model to any city or given area, and it allows the people of that place to work with the uniqueness of their geography and demography. I believe it is a really helpful and holistic model when thinking about population and planetary health.
There are then several aspects if a group wish to move from understanding their region to bringing about transformative action. Kate calls these the 8 M’s.
The model then includes 4 really helpful sets deeper questions to create the framework around the local/global – social/ecological foundations.
Firstly – what does it mean for people to thrive within their own Geography?
Secondly, what does it mean for the local environment/ecology to thrive and regenerate?
Thirdly, how do the local people contribute to the wellbeing of the wider family of humanity? How can they ensure they are good global citizens?
Fourthly, how does the locality contribute to the wellbeing of the whole planet, by how it behaves?
This way of working takes serious collaboration, co-production and real change-making. I love the way that Kate illustrates this:
Here in Morecambe Bay, we would employ things like ‘The Poverty Truth Commission’ and ‘The Art of Hosting’ to ensure that every voice is heard and we embrace ‘otherness’. It will involve partnership with the team at ImaginationLancaster, The Social Inequalities Research Centre and the Health Innovation Campus at Lancaster University, Cumbria University, The Eden Project and anchor institutions like our District Councils, County Councils, the NHS, BAE, EDF, School Federations, the CVFS and the network of SMEs. It will also mean developing the kind of culture I talk about here.
Out of the ashes of this devastating time, a phoenix can rise of a regenerated society and ecology. Are we up for it? I sincerely hope so and I wonder in how many places this can become possible. We need to create online and then, once lockdown is over, more real, radical spaces of hospitality and collaboration as we work together for the future that is calling us.
I’ve been thinking about how people can best use their time, if they are stuck at home during this Corona Virus, Covid-19 Pandemic. Some people will be asked to ‘self-isolate’, along with their household for 14 days because they have symptoms of a high temperature and/or a persistent and troubling cough. Others will be asked to do the same for 12 weeks if they are pregnant, over 70, or usually receive a flu-jab on the NHS (due to having an underlying health condition or on medication that suppresses their immune system). The reason for all of this is to try and suppress the spread of this virus, and maintain health in the wider community until we are sure we have better treatments and a vaccine that we can use across the population. Obviously, if you’re unwell, the first priority is to give your body time to recuperate by taking plenty of fluids (2-3 litres of water per day), eating well, sleeping and letting your immune system do it’s job, whilst you take paracetamol (at the recommended dose) to control your temperature and levels of pain. For many people, however, this time may feel frustrating, because symptoms will be mild or absent and some will be wondering what to do with the time they have been ‘gifted’.
There are 4 things, which I believe we can all do during this time, if we find ourselves in the situation of being in isolation, but not actually feeling too unwell.
REST
REFLECT
RE-IMAGINE
RESET
REST
This is something which we tend to not be very good at. However, we have been given the opportunity to step back from the fast-paced, consumerist-approach that we have adopted in society and take some time to just BE. Learning to accept that we are where we are and deliberately slowing down will enable us to find new strength and reconnect with that which is most important. Deliberately slowing down our breathing, our pace of walking and learning to calm our racing thoughts allows us to enter into a different mindset. Choosing to turn off our screens and disconnect from social media for good portions of the day allows us to create space in our heads and our hearts for another way of being. I know that social media can be a really important and safe space for many people to continue to connect and feel part of community, breaking down a sense of isolation and loneliness, but if we’re on there all the time, it can really fill our heads with unhelpful traffic and noise, which stops us being able to enter rest. As we rest, we are invited to spend our time differently – to do things that are good for the soul. You could take time to create, write, read, sing, dance, pray, go for a gentle walk, cook, sit round a table and build Lego or do jigsaws with others or on your own. There is no need to accumulate new things, what can you make do with or mend? What old or new hobbies might you rediscover or pick up? How about deliberately choosing not to get a thousand and one jobs done around the house or not rushing into a new decorating project. Just stop for a while, slow-down and rest.
REFLECT
When we consider the far reaching potential effects of a global pandemic, like the one we find ourselves in, it causes us to pause, notice more the interconnectedness of human life across the world and the utter fragility of our systems. It should cause us to notice more deeply the injustices upon which we build our society, the insecurity of work and the implications of global capitalism on the poorest in our communities and indeed our environment. During this time, we do well to reflect on what we are learning together. Birds are heard singing for the first time in years in Wuhan – a city usually thick with smog. Destructive air pollution has reduced by over 25% in China and Italy. The canals are cleaner than ever in Venice and global air travel has decreased significantly. Of course, we notice some of the worst bits of our humanity – driven by fear – and some selfishness. But we also see the indomitable human spirit at work – huge acts of love, courage, kindness and generosity. There are amazing offers to help and support with home schooling and teachers are going above and beyond their usual brilliance, thinking creatively about how best to enable their students to thrive. Healthcare workers continue to put themselves at risk and pour themselves into the work of healing. Voluntary food clubs to feed the hungry, delivery services for shopping and medication, community support schemes and the ongoing service of the most vulnerable in our society – it’s amazing. This ability to re-organise ourselves, to connect together differently, to make wider political and economic decisions and find a way to be that feels more wholesome should give us plenty not only to be grateful for but to reflect on about why we put so much energy into maintaining the usual status quo. What good things are we noticing and learning?
RE-IMAGINE
What might be possible together? Can we imagine a world with less commutes and more digital connection? Doesn’t it seem more possible to cut global emissions a great deal more quickly, when we’re forced to focus our attention? Could we work and earn differently and be more generous with wages and leave, so that we don’t see so many people left in such a vulnerable state. If we can find the ability to be so kind to each other at such a time as this – why not more so all the time? As we’ve recognised the fragility of our lives and existence, are the grudges we hold worthwhile? Are we able to forgive and reconnect? Might we adopt a way of life that is more about sharing and regenerating than grabbing all we can? Isn’t community one of the most delicious and richest of experiences? How can we build more of it? Can you sniff an economics that is more about wellbeing than profit and a politics that is more about connection and participation in our life together than centralised sovereignty? How about an education system that doesn’t treat our children like fodder for the machine, but invests in their ability to build a beautiful future. Have you seen how relationship really could be the foundation of our public services? So how might we think differently about our governance structures and the way we organise ourselves – think ‘Radical Help’ (Hilary Cottam), ‘Doughnut Economics’ (Kate Raworth) and ‘All Our Welfare’ (Peter Beresford) – plus many more. Can you imagine a society in which we really put the wellbeing of all people and the planet at the heart of what we do? If so….why would we continue with a way of being together which is so detrimental to both?
RESET
Our invitation, therefore, is to reset. This invitation comes from the earth itself, from our deepest longings, and from the source of all love and life itself. We don’t have to continue living in the story of selfishness and scarcity. We have shown ourselves that there is a more ancient and wonderful story of connectedness, restoration and hope, to which we all belong. We don’t have to go back to how it has been. Step by step, we can use this ‘kairos’ moment to walk into a new future together. A future in which we heal our divides and regenerate our planet, forgive our deep, historical wrongdoings, rebuild our ruins and restore our relationships; do away with injustice and create reconciliation. It’s time to reset. Are you ready to press the button?
Here is a beautiful poem, by Kitty O’Meara, to help us rest, reflect, re-imagine and rest.
In the last two blog posts on this subject, I’ve looked at the work of John Paul Lederach and Valerie Fournier in thinking about how change occurs in society. I’m returning to Lederach in this blog, to think about the next phase in social change – something, he calls “anchor points”.
Anchor points are people, places or communities to whom change has happened and who are on with the journey of starting alternative moral economies/experiments. They become anchors when they are rooted in a geography or set of relationships, which gives them a sense of longevity and consistency. Once infected with the virus that things cannot remain as they are, an anchor becomes a place where people dig deep, willing to make mistakes, to try new things, to fail early, to learn and to try again. This mixture of humility, bravery and innovation is vital if change is really going to begin to embed.
It begins to become really exciting, when anchor points connect. When a few people or communities within a given geography or inspired by the same hopes begin to connect, then the anchoring becomes even stronger. The space between the anchors, which some call transitional space or liminal space, becomes the place for strengthening and encouragement, but also the substantial reality in which the change begins to take place. My friend, Michael Schiffman sees it this way: “It’s like the emergent social change is of a particular colour. The hope of the social movement is not to take over the current institutions and try and lead them differently. Rather, the colour of the movement begins to flow into everything around it – communities, institutions, all facets of society. As it does, it begins to transform those spheres by infusing and diffusing its colour into and through them.” The change begins to happen almost unconsciously – and this is where one of two things can begin to occur: transformation or resistance.
Hitting against resistance is tiring and can feel intimidating. This is why anchor points need each other so much. They must hold each other, have each other’s backs, speak well of one another, believe the best and hold onto hope. They must continue to do their own inner work and stay true to the values which they hold. AND importantly (as Hilary Cottam taught me), they must learn what they are saying no to, as much as what they are saying yes to. As they do this, they will find fresh opportunities to bring change. My friend Roger MItchell talks about this around the concept of ‘Kenarchy’, which literally means the emptying out of power, or self-giving, others-empowering love. In his work, ‘church, gospel and empire’, he looks at love as an antidote to power. Social change, he argues, happens through a three-fold pattern of subversion, submission and substantiation. In other words, social change happens, as per Fournier, through outrage and challenging the inevitability of current social norms (subversion); creating moral alternative economies – but situated in the current realities – not somewhere or somehow separately (submission); and then making those things real in that context and thereby giving them grit/substance in every day life – anchoring them in communities (substantiation).
Once a social movement becomes substantiated it really begins to effect wider change. It has found enough momentum to begin to saturate it’s context with a new possibility that is no longer a dream on the horizon but a truly alternative way of being in the here and now. At this point it will either be resisted more forcefully, in which case, it has to become even more resilient and anchored, or it will begin to change and effect every level of society, including the very important arena of policy and governance. The biggest danger to the movement at this point is that it becomes subsumed, commodified and severely compromised by those powers who do not really want it bring about radical change and therefore alter it enough to still look a bit like radical change, but in actual fact simply ensure it serves the status quo, but in another guise! Resist and keep on loving!
I am hugely passionate about how we create great cultures in which to live and work. One particular thing I love is building a culture of joy! My friends Rachel Pilling and Dan Wadsworth have come up with a super easy way in which to practically build joy in work, through this simple but excellent idea of 15-30. This is the magic that happens when clinicians and managers work together. Watch it, if you work in the NHS then sign up and get involved and if you work outside the NHS – the idea is entirely replicable in any other part of life. By you going the extra mile now, you could save your friend a marathon….Building joy in work is, according to the IHI, the most important foundation on which to build a safe, sustainable and excellent health and care system. With staff morale as low as it is, let’s do what we can to promote joy in the daily grind. Here are Dan and Rachel explaining more in their excellent TEDxNHS talk – well worth your time!:
This question has become extremely important to me, in my work around how we tackle health inequalities and social injustice. It’s all too easy to take sides, point fingers and play the blame game. But if our political system teachers us anything, it is that this kind of didactic, oppositional approach to life, brings about little change, if any.
Over the last few years in Morecambe Bay, we’ve been exploring the power of Social Movements and how we can best work with our communities to effect real and lasting change. As, I said in part one of this series, we’ve been very affected by the need for personal change and the need for deep listening. Change begins with us and this requires genuine humility and deep listening, putting ourselves into uncomfortable situations and surroundings. How can we possibly make decisions for communities with whom we have never spent any time? It’s important that we do our own work and reflect on what we hear and be willing to change our way of working as a result. Series 3 of The Crown, highlights this beautifully with the inauguration of Prince Charles as The Prince of Wales. His relationship with his Welsh tutor utterly transforms the way he sees the plight of the welsh people and indeed his understanding of power, but it only comes from being immersed in Wales and having some significant challenge brought to his world-view.
Personal change does not just happen through encounters. The encounter with ‘the other’ invites us into a deeper journey of change. It’s why I have personally also found The Enneagram to be such a helpful tool when it comes to dealing with my own internal issues and mechanisms. For me, as a type 7, it has helped me to understand why I run away from pain and needlessly distract myself from the present in search for ever more stimulation. I have had to face this head on, in order to learn to become more fully human and the best gift I can be (nowhere near there yet!)….
I believe we will not see societal change if we are not, ourselves, willing to be changed. Personal transformation, however, is not enough, vital though it is. In thinking about wider social change, I have been really influenced by the philosopher, Valerie Fournier. She talks about three key components which are necessary to drive change within communities. Firstly, she says we must cultivate anger. Initially this seems like quite a strong statement, but what she is referring to is the need to stir a corporate sense of passion around injustice. I have certainly found this to be an important aspect of enabling change in our communities. If we’re not careful, we can spend much of our waking life asleep. If we are to be truly woke to the issues we’re facing across our communities then we must create a space in which people can become stirred to care enough about the reality of the status quo. We have found that people across Morecambe Bay really care about the fact that people living only a few miles apart can have a 15 year difference in life expectancy and an even bigger gap when it comes to years lived in good health. Our experience is that if we give no voice to the discontent within the communities, especially for those at the receiving end of systemic injustice, then we can end up going round in circles, unable to move forward. We definitely don’t want to remain in the place of anger, but it can be harnessed as an incredible energy for good.
The expression of anger is an important part of The Poverty Truth Commission process. Those who are subject to poverty and at the receiving end of the coldness of ‘the system’ need to be given voice to express what that means for them and how it impacts their sense of wellbeing. I think in Britain, we’re not particularly good at ‘anger’. It’s uncomfortable for us. It doesn’t feel polite. We would much rather keep things under wraps and hide away that which makes us feel ashamed. However, when we choose to be present enough to suspend what we think we know about poverty and the experience of it, and really listen to the harrowing reality of it, in another human being and then go on to build relationship and even friendship with that person….then we too are invited into that same anger, not to rage against the machine, but to use the power of our ‘fileo’ (friendship) love to become an agent of radical change.
Anger harnessed in this way leads to Fournier’s second step in social change: ‘Challenge inevitability’ – challenge the inevitability that things must always be this way. When we think about issues like poverty, health inequality, social injustice, adverse childhood experiences – things which feel ‘too hard to change’, it’s easy to resign ourselves to the notion that things will always be this way – therefore we should just ‘keep calm and carry on’, and just do what we can to ‘help those less fortunate than ourselves’….but all this does is reinforce the same old story. Social change requires that we challenge the inevitability of the status quo and that means challenging the world views we hold and the stories we tell ourselves. It doesn’t mean that we must therefore create a greater division between rich and poor or make enemies of ‘the elite’. It’s about taking ideologies that we hold to be ‘true’ and asking probing questions of them. In fact, it’s about giving them a really good shake and uprooting those that are deeply damaging and throwing them on the fire. There are great examples of this kind of work in economics – Kate Raworth in her book ‘Doughnut Economics’, or Katherine Trebeck in her book ‘The Economics of Arrival’ – both challenging economic theory built on GDP and obsessed with growth. We see it in Hilary Cottam’s tour de force ‘Radical Help’ in her challenge to the transactional basis of the welfare state. Bev Skeggs and Imogen Tyler, sociologists both challenging the way society is set up. Rob Barratt, challenging the way we think about education.
At the same time as challenging inevitability we just also incept our thinking with possibility of an alternative future, asking ourselves some powerful ‘what if?’ questions. I wonder what an economy might be like if it held wellbeing of people and the planet as it’s core principles? – a question they are asking in Scotland, New Zealand and Iceland. What if we had a society in which women (change women for any other subjugated group) were treated as true equals? I wonder what education might be like if it were truly future orientated and took climate change seriously? If we challenge what is, it allows us to reimagine what might be.
New ideas though, are not enough. The undermining of our current realities opens up the possibility for Fournier’s third aspect of social change, which is to ‘Create moral alternative economies’. We must move from anger and challenge, into experiment. Appreciative Enquiry is a great approach to help us move into this space. It allows communities to focus on what is strong, rather than what is wrong. If we’re going to experiment with new ways of building society, politics, economics etc, we need to so on strong foundations. Once we have cleared the ground in our minds of what has been stopping us find kinder ways forward, we can then focus in on – ok – so what is good?
As a result of this approach in the Poverty Truth Commission, for example, we’ve been able to work together on designing the kind of job roles that would really help someone navigate the complexities of the health, social care and welfare system, when they are on the ropes. We heard the anger about where it isn’t working, challenged our own thinking that we can’t really change things and have begun to experiment with the ideas put forward by people on the receiving end of unkind and punitive processes. We’re creating a moral alternative economy. When our city council in Lancaster, recently voted to protect the rights of gypsy-travellers by buying their land and promising to ensure it is fit to live on – they also responded to the anger of deep injustice at what was being proposed (the selling of their land), challenged the inevitability that they had no choice in solving the matter and instead intervened with a moral alternative economy, that protected the ‘poor’ and actually worked for the benefit of everyone. Or, we could take an example from education: When a teacher refuses to tow the line to isolate a student and have them face a wall all day and instead finds a more creative way to understand their student’s anger, challenging the inevitability of school exclusion (and all that will lead onto) and finds an alternative way to help them process their trauma and make the system work for them, rather than the other way round – that teacher is creating a moral alternative economy. You see? We can begin to do it everywhere! And when we begin to experiment with new ways of being together in communities, we begin to tell each other a new and altogether more loving story than the one we’re currently living in. The more we experiment and either fail or succeed, the more we discover how to build a society that works for the wellbeing/peace of everyone and the planet.
So, where do you need to listen more deeply, to allow yourself to be made uncomfortable by the palpable anger that is underneath the surface, or sometimes erupting onto our streets? Why is the anger there? What does it tap into? Where is it coming from? Who is it aimed at? Is that anger able to be channelled in a way that can leverage an altogether more loving and kind society? What inevitability in your personal or our corporate thinking needs to be challenged as a result? What ‘truths’ need to be questioned? What space might that clear for new experiments to emerge? What if those experiments began to interconnect and learn from each other, sharing resources and encouragement along the way? What might then become possible? What if we actually took a breath and decided to genuinely think and work in this way? Can you see the change ahead?! Go ahead and start creating it!







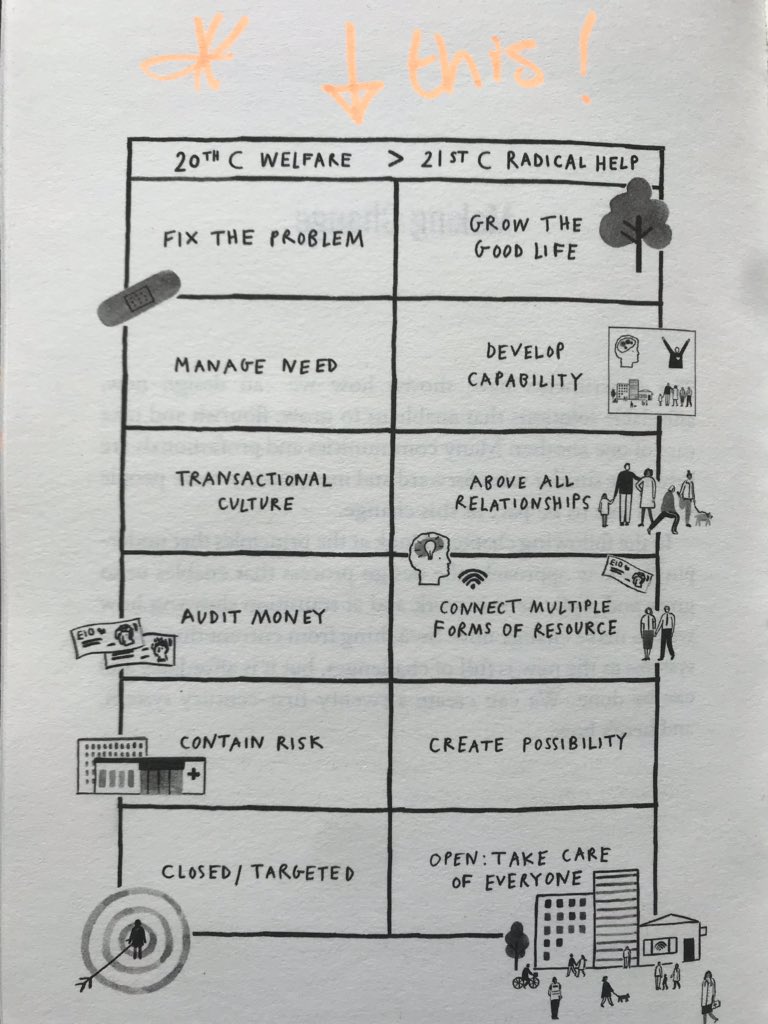




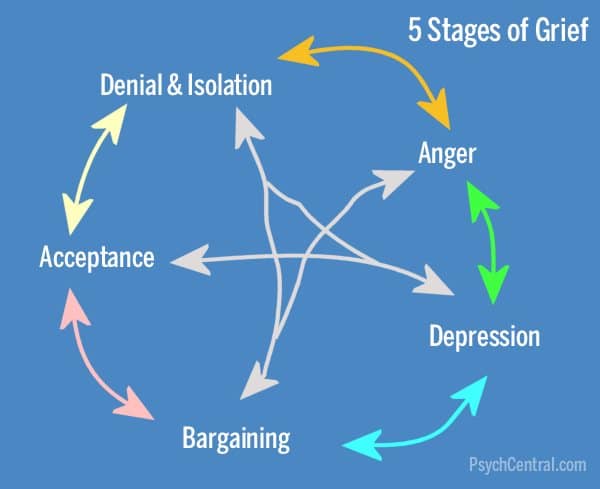
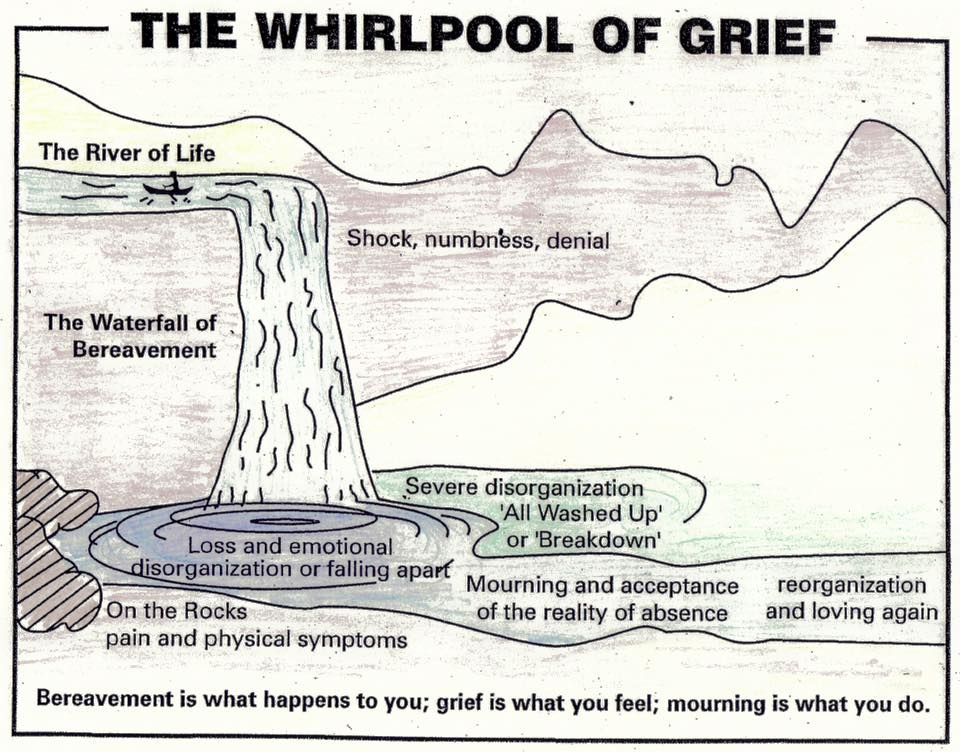

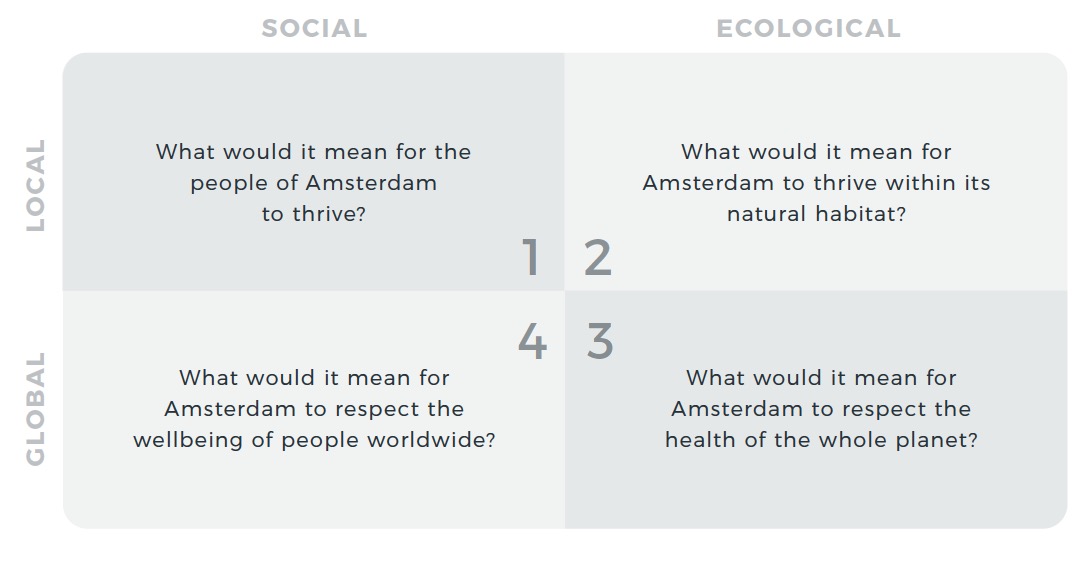
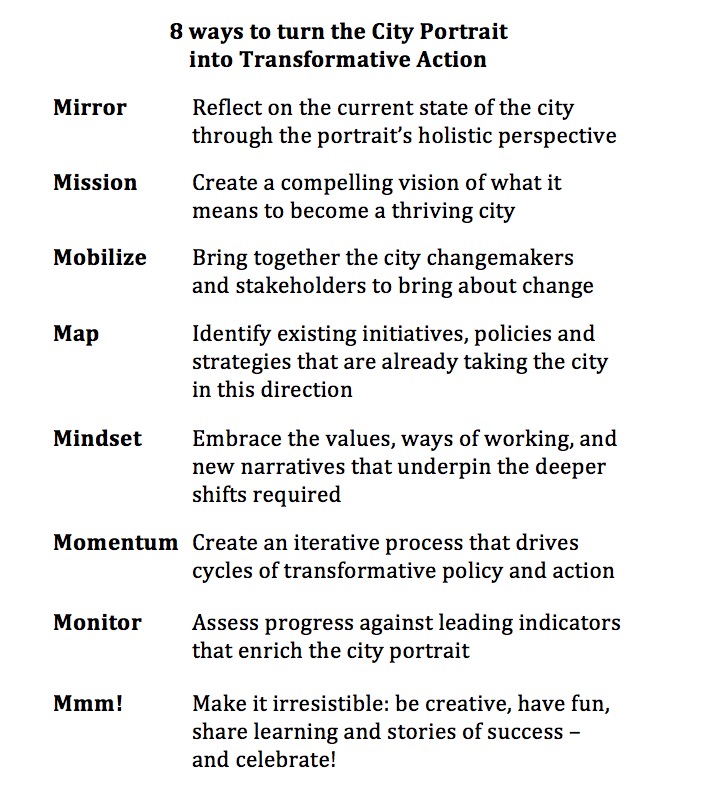
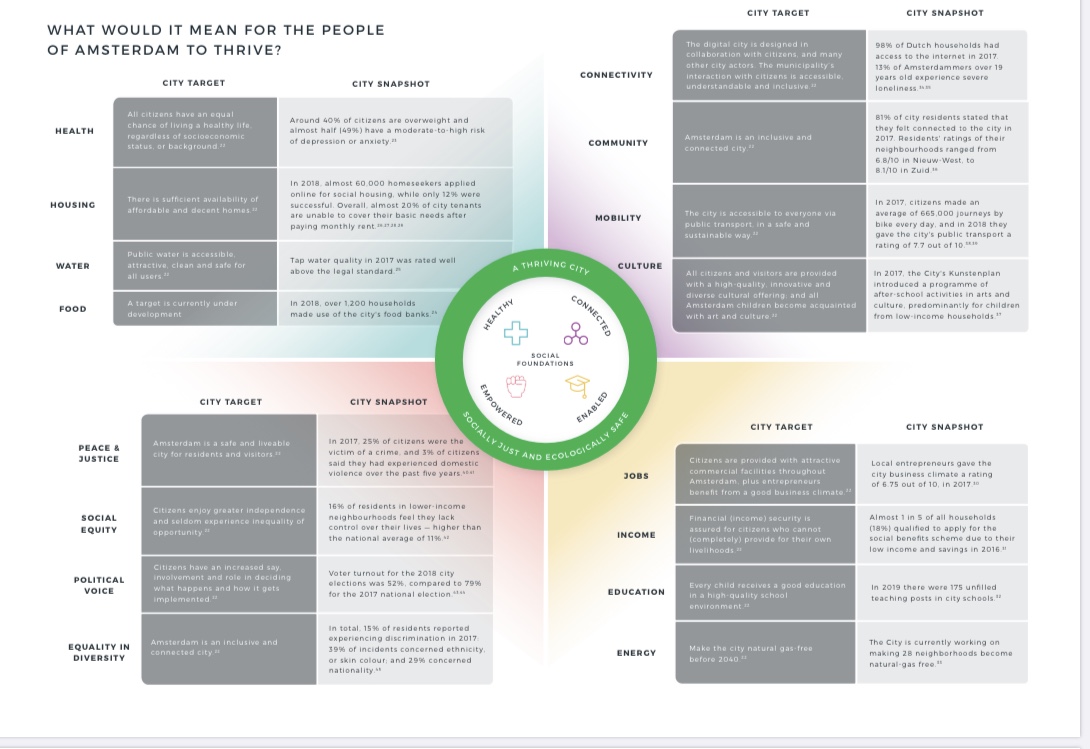
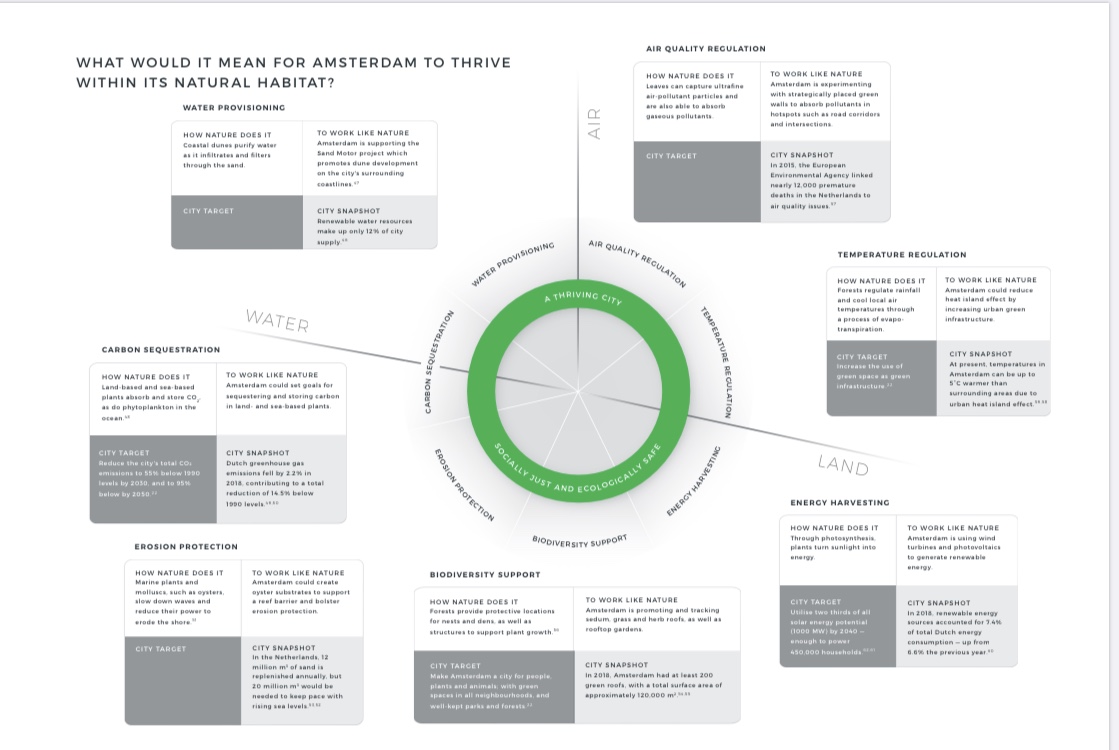
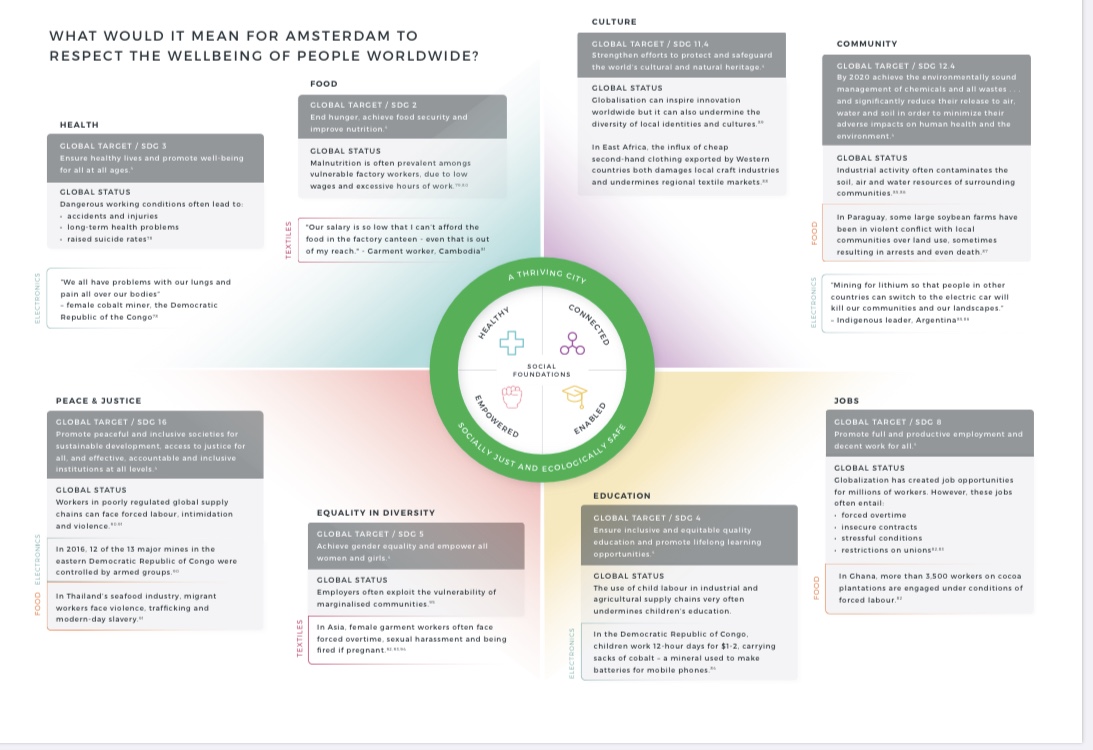
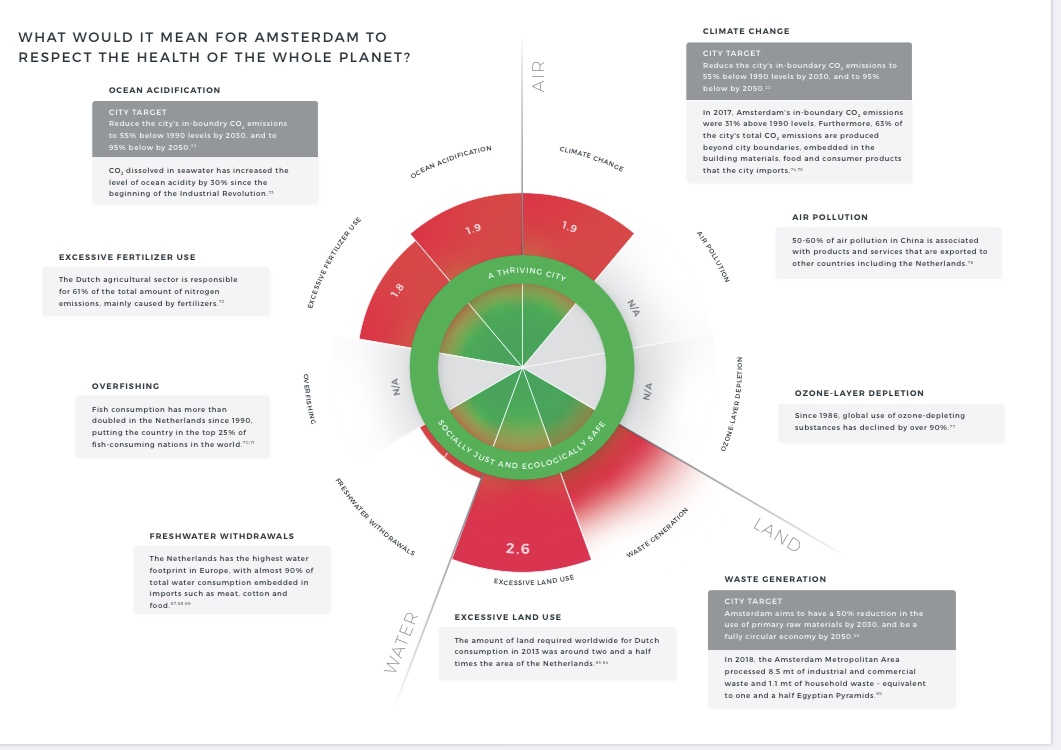
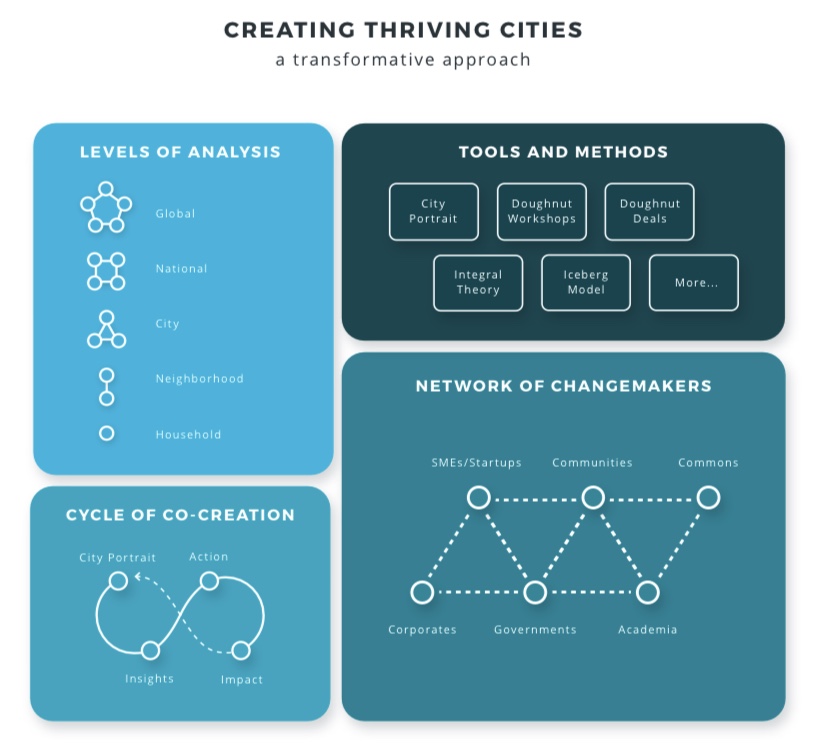









{kind=link}
 – Breaking The Stigma, Finding The Solutions){kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}